
Rationale and Objectives
The goal was to determine discordance rates between preliminary radiology reports provided by on-call radiology house staff and final reports from attending radiologists on cross-sectional imaging studies requested by emergency department staff after hours.
Materials and Methods
A triplicate carbon copy reporting form was developed to provide permanent records of preliminary radiology reports and to facilitate communication of discrepant results to the emergency department. Data were collected over 21 weeks to determine the number of discordant readings. Patients’ medical records were reviewed to show whether discrepancies were significant or insignificant and to assess their impact on subsequent management and patient outcome.
Results
The emergency department requested 2830 cross-sectional imaging studies after hours and 2311 (82%) had a copy of the triplicate form stored in radiology archives. Discrepancies between the preliminary and final report were recorded in 47 (2.0%), with 37 (1.6%) considered significant: 14 patients needed no change, 13 needed a minor change, and 10 needed a major change in subsequent management. Ten (0.43%) of the discordant scans were considered insignificant. A random sample of 104 (20%) of the 519 scans without a paper triplicate form was examined. Seventy-one (68%) did have a scanned copy of the triplicate form in the electronic record, with a discrepancy recorded in 3 (4.2%), which was not statistically different from the main cohort ( P = .18).
Conclusion
Our study suggests a high level of concordance between preliminary reports from on-call radiology house staff and final reports by attending subspecialty radiologists on cross-sectional imaging studies requested by the emergency department.
Cross-sectional imaging plays an essential diagnostic role in the evaluation of patients presenting to the emergency department (ED). In the majority of academic institutions, the on-call radiology service is primarily provided by radiology residents, with back-up coverage from board-certified radiology fellows and attending subspecialty radiologists. Preliminary interpretations are rendered to the ED by the on-call resident, with the final reading being provided by a subspecialty radiology attending the following morning. Residents are often required to interpret complex cross-sectional imaging studies and independently make decisions, and this valuable on-call experience is considered an integral part of radiology residency training. However, emergency physicians and trauma surgeons have expressed concerns about the reliability of preliminary radiology reports provided by residents and believe that around-the-clock radiology attending coverage is essential to prevent errors in the management of patients presenting to the ED ( ). Other quality concerns include the timeliness and manner in which discrepant results are conveyed to the ED and whether the discrepancy is accurately documented within the final radiology report or patient’s records ( ). Without a clear protocol for ensuring that this information and its subsequent affect on patient management are accurately entered into the patient’s medical record, patient care may be adversely affected.
Previous studies have shown a wide variation in reported discrepancy rates between preliminary reports provided by the on-call resident and final reports from the subspecialty attending radiologist, ranging from 3% to 29.9% ( ). Although several studies have examined the significance of such discrepancies on subsequent patient care and eventual outcome ( ), no attention has been focused on how quickly or effectively the discrepancy was communicated to the ED staff.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Setting
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
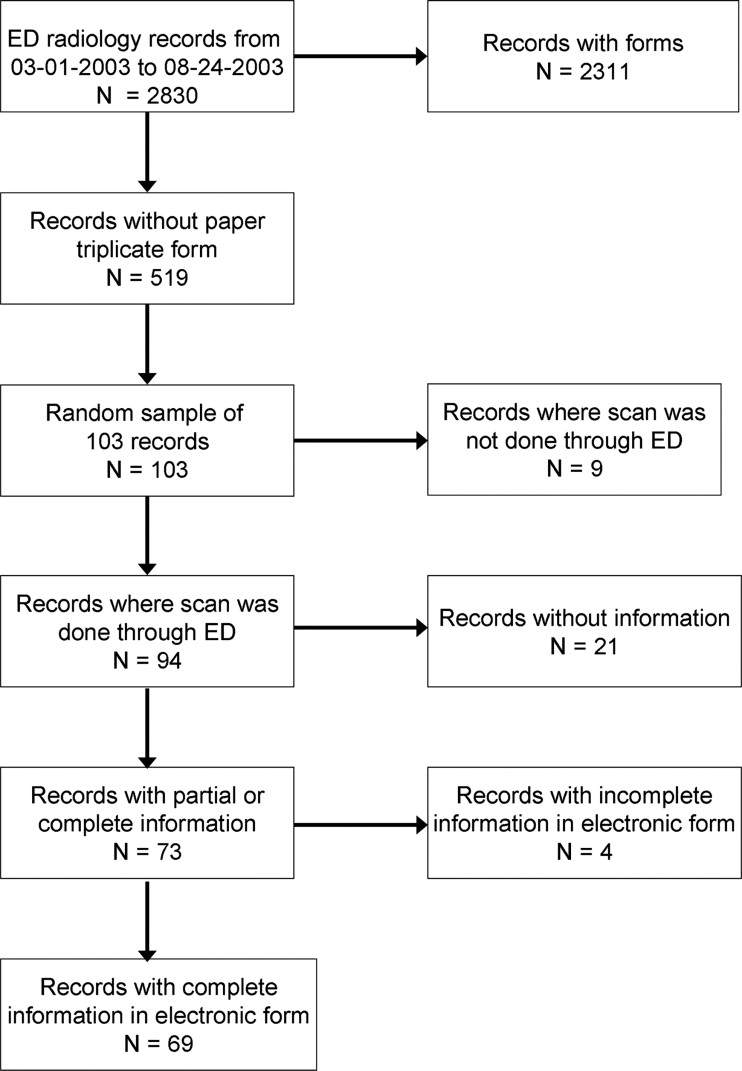
Table 1
Classification of Discordant Scan Results
Grading of Discordant Scan Results Significant ⁎ Insignificant † Total 37 (1.60%) 10 (0.43%) No change in treatment 14 (0.61%) 10 (0.43%) Minor change in treatment ‡ 13 (0.56%) 0 Major change in treatment § 10 (0.43%) 0
Number of discordant scans (percentage of 2311 scans performed).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Scans With a Significant Discrepancy Between the Preliminary and Final Reports Requiring a Major Change In Management
Age (yr) Sex Presenting Complaint Scan Provisional Scan Report Brief Description of Discrepant Finding Between Provisional and Final Report Initial Clinical Management from ED Change in Clinical Management Following Final Scan Report Expected Change in Treatment if Final Report Was Available When Patient Was in ED Time Between Scan Reports (h) 20 Male Fell off bike, hitting abdomen on handlebars CT abdomen/pelvis Abnormal (small hematoma rectus sheath) Subtle small bowel edema and thickening, possible bowel injury Discharged home No further record in patient notes Would have been admitted 8.5 25 Female Acute abdominal pain and low-grade fever CT abdomen/pelvis Normal Appendicitis Discharged home Called back to ED for reassessment 12 h later. Admitted and underwent laparoscopic appendectomy within 4 h. Would have been admitted/surgery 4.75 63 Female Abdominal pain, constipation CT abdomen/pelvis Abnormal (gallstones) Possible early pancreatitis Discharged home Patient contacted, visiting her sister, message left. No further contact recorded Would have been admitted 14 84 Female Intermittent abdominal cramps, past history of ovarian ca with TAH and BSO CT abdomen/pelvis Abnormal (fluid collection in pelvis? diverticular abscess) Pelvic mass, likely neoplasm, no abscess Admitted to surgeons, with diagnosis of pelvis abscess. Commenced on IV antibiotics Gynecology referral. Scheduled for surgery 3 d later but delayed for 7 d as INR too high. Surgery showed recurrent ovarian cancer. Subspecialty referral/change in treatment 10.75 6 Male Hit on head with baseball bat CT head Abnormal (fracture left orbital rim) Possible pneumocephalus in right spenoid sinus, right medial orbital wall fracture Discharged to plastics for suturing and subsequently discharged home same day. No further record in patient notes Further imaging/would have been admitted 14.25 14 Male Fell off bike, head injury with 1 min loss of consciousness CT head Normal Possible small temporal lobe contusion Discharged home Patient contacted. Asymptomatic, advised to see PCP as planned Subspecialty referral 16.5 54 Female Sudden onset severe headache during exercise CT head Normal ACOM aneurysm Discharged home, with neurology follow-up next morning Neuroangiogram performed 13 d later, with aneurysm clipping 43 d later Would have been admitted 13.5 69 Female Left facial pain and weakness CT head Normal Possible aneurysm near left MCA/ICA Discharged home Patient had MRI scan confirming aneurysm, but also showed left frontal menigioma, resected 7 days later Further imaging/subspecialty referral 19.5
ACOM, anterior communicating artery; BSO, bilateral salpingo-oophorectomy; CT, computed tomography; ED, emergency department; ICA, internal carotid artery; MCA, middle cerebral artery; PCP, primary care physician; TAH, total abdominal hysterectomy.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Variation of Discordance Rates With Type of Examination and Radiologic Subspecialty
Type of Scan Subspecialty All Neuroradiology Body Angiography Computed tomography All scans 1125 738 172 2035 Discordant scans 23 20 2 45 (2.21%) Ultrasound All scans 8 245 1 254 Discordant scans 0 2 0 2 (0.79%) Magnetic resonance imaging All scans 18 2 2 22 Discordant scans 0 0 0 0 (0%) All All scans 1151 985 175 2311 Discordant scans 23 (2.00%) 22 (2.23%) 2 (1.14%) 47 (2.03%)
Table 4
Generalized Linear Regression (Binomial Family, Loglog Link) of Discordance on Scanning Factors ( N = 2192)
Variable Odds Ratio SD_z__P_ > | z | Odds Ratio (95% confidence interval) Scan type MRI ⁎ versus CT 0.24 11.37 −0.03 0.976 3 e −42 2 e +40 Ultrasound versus CT 0.73 0.12 −1.95 0.051 0.53 1.00 Scan area Body vs. neuroimaging 1.11 0.09 1.25 0.210 0.94 1.31 Angiographic vs. neuroimaging 0.89 0.15 −0.71 0.480 0.64 1.24 Weekend 1.13 0.10 1.35 0.178 0.95 1.34 Time period Evening versus day 1.20 0.16 1.43 0.154 0.93 1.55 Night versus day 1.12 0.15 0.85 0.398 0.86 1.44
CT, computed tomography; MRI, magnetic resonance imaging.
Deviance = 437, Akaike information criterion = 0.207, Bayesian information criterion = −16363.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Confidence Intervals for Patients With a Discrepancy Between the Preliminary and Final Report
Situation_N__n_ % 95% Confidence Interval Discordance in cases with forms 2311 47 2.03 1.50–2.70 Significant discordance in cases with forms 2311 37 1.6 1.13–2.20 Immediate management change in cases with significant discordance 2311 10 0.43 0.21–0.79 Discordance in cases without paper forms, but copy in electronic notes 71 3 4.23 0.88–11.86
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 6
Generalized Linear Regression (binomial family, log-log link) of Presence of Paper Form on Scanning Factors ( N = 2711)
Variable Odds Ratio SD_z__P_ > | z | Odds Ratio (95% confidence interval) Scan type MRI ⁎ versus CT 0.20 0.05 −6.81 0.000 0.13 0.32 Ultrasound versus CT 0.24 0.03 −11.08 0.000 0.19 0.31 Scan area Body vs. neuroimaging 6.88 0.92 14.51 0.000 5.31 8.93 Angiographic vs. neuroimaging 0.30 0.03 −13.83 0.000 0.00 0.36 Day of week Monday vs. Sunday 1.25 0.15 1.89 0.058 0.99 1.57 Tuesday vs. Sunday 1.09 0.13 0.80 0.423 0.88 1.37 Wednesday vs. Sunday 1.29 0.15 2.14 0.032 1.02 1.62 Thursday vs. Sunday 1.50 0.18 3.43 0.001 1.19 1.89 Friday vs. Sunday 1.10 0.13 0.81 0.417 0.88 1.38 Saturday vs. Sunday 1.12 0.11 1.20 0.230 0.93 1.35 Time period Evening vs. day 0.82 0.08 −1.92 0.054 0.68 1.00 Night vs. day 0.79 0.08 −2.39 0.017 0.65 0.96
CT, computed tomography; MRI, magnetic resonance imaging.
Deviance = 1776, Akaike information criterion = 0.665, Bayesian information criterion = −19,551.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Table 7
Comparison of Major and Minor Discordance Rates in Similar Studies
Authors Year No. of Cases Discrepancies (%) Major Minor Roszler et al. ( ) 1991 289 2.1 2.1 Wechsler et al. ( ) 1996 598 1.2 6.5 Wysoki et al. ( ) 1998 419 1.7 2.6 Lal et al. ( ) 2000 2388 0.5 0.4 Velmahos et al. ( ) 2001 383 5.0 11.0 Erly et al. ( ) 2002 1324 2.0 7.0 Yoon et al. ( ) 2002 512 2.3 26.6 Carney et al. ( ) 2003 928 0.5 3.2 Erly et al. ( ) 2003 716 2.0 2.9 Present study 2003 2311 1.6 0.43
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Blane C.E., Desmond J.S., Helvie M.A., et. al.: Academic radiology and the emergency department: Does it need changing?. Acad Radiol 2007; 14: pp. 625-630.
2. Levine C., Hirschorn D., Baker S.R.: Radiology coverage 24/7—What can we do, who can we call?. Emerg Radiol 2003; 10: pp. 119-120.
3. Lowe R.A., Abbuhl S.B., Baumritter A., et. al.: Radiology services in emergency medicine residency programs: A national survey. Acad Emerg Med 2002; 9: pp. 587-594.
4. Rogers L.F.: Heeding the call: Radiologists in the ED (emergency department). AJR Am J Roentgenol 2000; 175: pp. 1213.
5. Velmahos G.C., Fili C., Vassiliu P., Nicolaou N., Radin R., Wilcox A.: Around-the-clock attending radiology coverage is essential to avoid mistakes in the care of trauma patients. Am Surg 2001; 67: pp. 1175-1177.
6. Stubbs D.M.: Emergency radiology services at medical schools in the United States. Invest Radiol 1992; 27: pp. 648-652.
7. Baker S.R.: Emergency radiology: Challenges and issues. Radiographics 1996; 16: pp. 935-938.
8. Baker S.R.: Call back or else. Emerg Radiol 2004; 10: pp. 233-234.
9. Albano M.C., Ross G.W., Ditchek J.J., et. al.: Resident interpretation of emergency CT scans in the evaluation of acute appendicitis. Acad Radiol 2001; 8: pp. 915-918.
10. Carney E., Kempf J., DeCarvalho V., Yudd A., Nosher J.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. AJR Am J Roentgenol 2003; 181: pp. 367-373.
11. Erly W.K., Ashdown B.C., Lucio R.W., Carmody R.F., Seeger J.F., Alcala J.N.: Evaluation of emergency CT scans of the head: Is there a community standard?. AJR Am J Roentgenol 2003; 180: pp. 1727-1730.
12. Erly W.K., Berger W.G., Krupinski E., Seeger J.F., Guisto J.A.: Radiology resident evaluation of head CT scan orders in the emergency department. AJNR Am J Neuroradiol 2002; 23: pp. 103-107.
13. Ginsberg M.S., King V., Panicek D.M.: Comparison of interpretations of CT angiograms in the evaluation of suspected pulmonary embolism by on-call radiology fellows and subsequently by radiology faculty. AJR Am J Roentgenol 2004; 182: pp. 61-66.
14. Hillier J.C., Tattersall D.J., Gleeson F.V.: Trainee reporting of computed tomography examinations: Do they make mistakes and does it matter?. Clin Radiol 2004; 59: pp. 159-162. discussion 157−158
15. Lal N.R., Murray U.M., Eldevik O.P., Desmond J.S.: Clinical consequences of misinterpretations of neuroradiologic CT scans by on-call radiology residents. AJNR Am J Neuroradiol 2000; 21: pp. 124-129.
16. Roszler M.H., McCarroll K.A., Rashid T., Donovan K.R., Kling G.A.: Resident interpretation of emergency computed tomographic scans. Invest Radiol 1991; 26: pp. 374-376.
17. Strub W.M., Leach J.L., Tomsick T., Vagal A.: Overnight preliminary head CT interpretations provided by residents: Locations of misidentified intracranial hemorrhage. AJNR Am J Neuroradiol 2007; 28: pp. 1679-1682.
18. Wechsler R.J., Spettell C.M., Kurtz A.B., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.
19. Wysoki M.G., Nassar C.J., Koenigsberg R.A., Novelline R.A., Faro S.H., Faerber E.N.: Head trauma: CT scan interpretation by radiology residents versus staff radiologists. Radiology 1998; 208: pp. 125-128.
20. Yoon L.S., Haims A.H., Brink J.A., Rabinovici R., Forman H.P.: Evaluation of an emergency radiology quality assurance program at a level I trauma center: abdominal and pelvic CT studies. Radiology 2002; 224: pp. 42-46.
21. Ruchman R.B., Jaeger J., Wiggins E.F., et. al.: Preliminary radiology resident interpretations versus final attending radiologist interpretations and the impact on patient care in a community hospital. AJR Am J Roentgenol 2007; 189: pp. 523-526.
22. Scott J.N., Romano C.C.: On-call services provided by radiology residents in a university hospital environment. Can Assoc Radiol J 2003; 54: pp. 104-108.
23. Bechtold R.E., Chen M.Y., Ott D.J., et. al.: Interpretation of abdominal CT: Analysis of errors and their causes. J Comput Assist Tomogr 1997; 21: pp. 681-685.
24. Wakeley C.J., Jones A.M., Kabala J.E., Prince D., Goddard P.R.: Audit of the value of double reading magnetic resonance imaging films. Br J Radiol 1995; 68: pp. 358-360.
25. Borgstede J.P., Lewis R.S., Bhargavan M., Sunshine J.H.: RADPEER quality assurance program: A multifacility study of interpretive disagreement rates. J Am Coll Radiol 2004; 1: pp. 59-65.
26. Carroll T.J.: Trends in on-call workload in an academic medical center radiology department 1998–2002. Acad Radiol 2003; 10: pp. 1312-1320.
27. Tellis W.M., Andriole K.P.: Integrating multiple clinical information systems using the Java message service framework to enable the delivery of urgent exam results at the point of care. J Digit Imaging 2005; 18: pp. 316-325.
28. Branstetter B.Ft, Morgan M.B., Nesbit C.E., et. al.: Preliminary reports in the emergency department: Is a subspecialist radiologist more accurate than a radiology resident?. Acad Radiol 2007; 14: pp. 201-206.
29. DeCorato D.R., Kagetsu N.J., Ablow R.C.: Off-hours interpretation of radiologic images of patients admitted to the emergency department: Efficacy of teleradiology. AJR Am J Roentgenol 1995; 165: pp. 1293-1296.
30. Eng J., Mysko W.K., Weller G.E., et. al.: Interpretation of emergency department radiographs: A comparison of emergency medicine physicians with radiologists, residents with faculty, and film with digital display. AJR Am J Roentgenol 2000; 175: pp. 1233-1238.
31. Kalyanpur A., Weinberg J., Neklesa V., Brink J.A., Forman H.P.: Emergency radiology coverage: Technical and clinical feasibility of an international teleradiology model. Emerg Radiol 2003; 10: pp. 115-118.
32. Pysher L., Harlow C.: Teleradiology using low-cost consumer-oriented computer hardware and software. AJR Am J Roentgenol 1999; 172: pp. 1181-1184.
33. Saketkhoo D.D., Bhargavan M., Sunshine J.H., Forman H.P.: Emergency department image interpretation services at private community hospitals. Radiology 2004; 231: pp. 190-197.