
Rationale and Objectives
To investigate the feasibility and performance of 7T magnetic resonance imaging compared to 1.5T imaging to discriminate benign (normal and inflammatory changed) from tumor-bearing lymph nodes in rabbits using ultrasmall particles of iron oxide (USPIO)-based contrast agents.
Materials and Methods
Six New Zealand White rabbits were inoculated with either complete Freund’s adjuvant cell suspension (n = 3) to induce reactively enlarged lymph nodes or with VX2 tumor cells to produce metastatic lymph nodes (n = 3). Image acquisition was performed before and 24 hours after bolus injection of an USPIO contrast agent at 1.5T and afterward at 7T using T1-weighted and T2*-weighted sequences. Sensitivities, specificities, and negative and positive predictive values for the detection of lymph node metastases were calculated for both field strengths with histopathology serving as reference standard. Sizes of lymph nodes with no, inflammatory, and malignant changes were compared using a Mann-Whitney U -test.
Results
All 24 lymph nodes were detected at 1.5T as well as at 7T. At 1.5T, sensitivity amounted to 0.67, while specificity reached a value of 1. At the higher field strength (7T), imaging was able to reach sensitivity and specificity values of 1. No statistical differences were detected concerning lymph node sizes.
Conclusions
Magnetic resonance lymphography with USPIO contrast agents allows for differentiation of normal and reactively enlarged lymph nodes compared to metastatic nodes. First experiments at 7T show promising results compared to 1.5T, which have to be evaluated in further trials.
The detection of lymph node metastases is part of nearly any cancer staging as lymph node involvement has a poor prognosis for many tumor entities and can directly impact a patient’s management .
Computed tomography (CT) and magnetic resonance imaging (MRI) are established tools for staging malignant tumors. A short-axis diameter of >10 mm has been the major malignancy marker for lymph node evaluation of many cancer types (e.g., uterine cervical and other pelvic cancer). On the basis of this technique, false-positive results may occur for reactively enlarged lymph nodes without metastatic infiltration as well as false-negative results if a lymph node shows (micro)metastasis (focal small tumor infiltration <2 mm) in a nonenlarged node . Therefore, new MRI techniques including diffusion-weighted MRI, high-field MRI, and contrast-enhanced lymphography have been evaluated in the past years.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Animal Model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Imaging Parameters for T1-Weighted and T2*-Weighted Sequences at 1.5T and 7T
Repetition Time (ms) Echo Time (ms) Flip Angle (°) Field of View (mm) Voxel Size (mm 3 ) Bandwidth (Hz/px) Time of acquisition (min:s) T2*-weighted 7T 1000 13 30 149 × 180 0.47 × 0.47 × 1.5
interpolated
0.23 × 0.23 × 1.5 435 2:30 T2*-weighted 1.5T 28 15 30 192 × 256 1.12 × 1 × 1.2
interpolated
0.56 × 0.5 × 1.2 500 2:20 T1-weighted 7T 6.12 2.63 10 157 × 180 0.4 × 0.35 × 0.5
interpolated
0.4 × 0.35 × 0.4 315 2:56 T1-weighted 1.5T 553 12 90 250 × 250 0.98 × 0.98 × 1.2
interpolated
0.49 × 0.49 × 1.2 130 2:21
Get Radiology Tree app to read full this article<
Histopathological Analysis
Get Radiology Tree app to read full this article<
MRI Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Histopathological Analysis
Get Radiology Tree app to read full this article<
MRL Analysis
Get Radiology Tree app to read full this article<
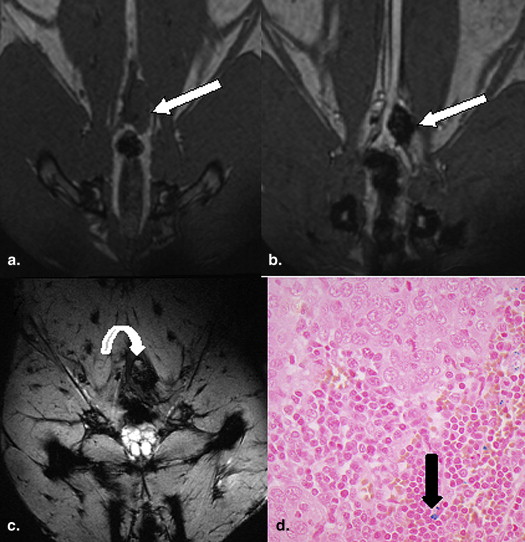
![Figure 1, A healthy lymph node ( arrow ) in the right popliteal fossa shown at 1.5T T2*-weighted imaging (multiple echo data image combination [MEDIC]; a) and T1-weighted imaging (b) 24 hours after contrast as well as on 7T T2*-weighted imaging (MEDIC, c) and T1-weighted imaging (d) . Note the different image aspects of the sequences due to different field strength and the high iron uptake of the nonaffected lymph node, which even turns it dark on T1-weighted imaging.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/DiscriminationofBenignandMalignantLymphNodesat70TComparedto15TMagneticResonanceImagingUsingUltrasmallParticlesofIronOxide/0_1s20S1076633213004121.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Sensitivity, Specificity, and Positive and Negative Predictive Values for 1.5T and 7T
1.5T 7T Sensitivity 0.67 1 Specificity 1 1 Positive predictive value 1 1 Negative predictive value 0.9 1
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kimura K., Tanigawa N., Matsuki M., et. al.: High-resolution MR lymphography using ultrasmall superparamagnetic iron oxide (USPIO) in the evaluation of axillary lymph nodes in patients with early stage breast cancer: preliminary results. Breast Cancer 2009; 17: pp. 241-246.
2. Yoshimura G., Sakurai T., Oura S., et. al.: Evaluation of axillary lymph node status in breast cancer with MRI. Breast Cancer 1999; 6: pp. 249-258.
3. Scheidler J., Hricak H., Yu K.K., et. al.: Radiological evaluation of lymph node metastases in patients with cervical cancer. A meta-analysis. JAMA 1997; 278: pp. 1096-1101.
4. Kim S.H., Kim S.C., Choi B.I., et. al.: Uterine cervical carcinoma: evaluation of pelvic lymph node metastasis with MR imaging. Radiology 1994; 190: pp. 807-811.
5. Harisinghani M.G., Barentsz J., Hahn P.F., et. al.: Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med 2003; 348: pp. 2491-2499.
6. Umutlu L., Kraff O., Orzada S., et. al.: Dynamic contrast-enhanced renal MRI at 7 Tesla: preliminary results. Invest Radiol 2011; 46: pp. 425-433.
7. Kraff O., Theysohn J.M., Maderwald S., et. al.: High-resolution MRI of the human parotid gland and duct at 7 Tesla. Invest Radiol 2009; 44: pp. 518-524.
8. Zwanenburg J.J., Hendrikse J., Visser F., et. al.: Fluid attenuated inversion recovery (FLAIR) MRI at 7.0 Tesla: comparison with 1.5 and 3.0 Tesla. Eur Radiol 2010; 20: pp. 915-922.
9. Korteweg M., Zwanenburg J., van Diest P., et. al.: Characterization of ex vivo healthy human axillary lymph nodes with high resolution 7 Tesla MRI. Eur Radiol 2011; 21: pp. 310-317.
10. Wu L., Cao Y., Liao C., et. al.: Diagnostic performance of USPIO-enhanced MRI for lymph-node metastases in different body regions: a meta-analysis. Eur J Radiol 2011; 80: pp. 582-589.
11. Kinner S., Maderwald S., Albert J., et. al.: Comparison of two different iron oxide–based contrast agents for discrimination of benign and malignant lymph nodes. Investig Radiol 2012; 47: pp. 511-515.
12. Wagner S.: Benign lymph node hyperplasia and lymph node metastases in rabbits. Animal models for magnetic resonance lymphography. Invest Radiol 1994; 29: pp. 364-371.
13. Dunne A.A., Kuropkat C., Sapundzhiev N., et. al.: Intravenous chemotherapy with cisplatin for regional lymph node metastases of auricular VX2 carcinoma. Anticancer Res 2004; 24: pp. 1785-1790.
14. Bennett B., Check I.J., Olsen M.R., et. al.: A comparison of commercially available adjuvants for use in research. J Immunol Methods 1992; 153: pp. 31-40.
15. Abduljalil A.M., Robitaille P- M.L.: Macroscopic susceptibility in ultra high field MRI. J Comput Assist Tomogr 1999; 23: pp. 832-841.
16. Wadghiri Y.Z., Johnson G., Turnbull D.H.: Sensitivity and performance time in MRI dephasing artifact reduction methods. Magn Reson Med 2001; 45: pp. 470-476.
17. De Guio F., Benoit-Cattin H., Davenel A.: Signal decay due to susceptibility-induced intravoxel dephasing on multiple air-filled cylinders: MRI simulations and experiments. Magn Reson Mater Physics. Biol Med 2008; 21: pp. 261-271.
18. Heesakkers R.A., Fütterer J.J., Hövels A.M., et. al.: Prostate cancer evaluated with ferumoxtran-10–enhanced T2*-weighted MR imaging at 1.5 and 3.0 T: early experience 1. Radiology 2006; 239: pp. 481-487.
19. Choi S.H., Kim K.H., Moon W.K., et. al.: Comparison of lymph node metastases assessment with the use of USPIO-enhanced MR imaging at 1.5-T versus 3.0 T in a rabbit model. J Magn Reson Imaging 2010; 31: pp. 134-141.