
Rationale and Objectives
A doxorubicin-loaded microbubble has been developed that can be destroyed with focused ultrasound resulting in fragments, or “nanoshards” capable of escaping through the leaky tumor vasculature, promoting accumulation within the interstitium. This study uses a rat liver cancer model to examine the biodistribution and tumoral delivery of this microbubble platform compared with de novo drug-loaded polymer nanoparticles and free doxorubicin.
Materials and Methods
Microbubbles (1.8 μm) and 217-nm nanoparticles were prepared containing 14-C labeled doxorubicin. Microbubbles, nanoparticles, a combination of the two, or free doxorubicin were administered intravenously in rats bearing hepatomas, concomitant with tumor insonation. Doxorubicin levels in plasma, organs, and tumors were quantified after 4 hours and 7 and 14 days. Tumors were measured on sacrifice and evaluated with autoradiography and histology.
Results
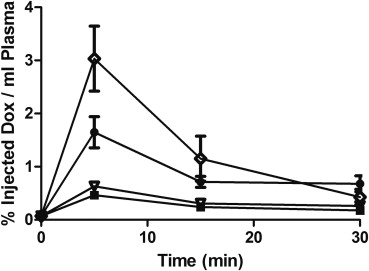
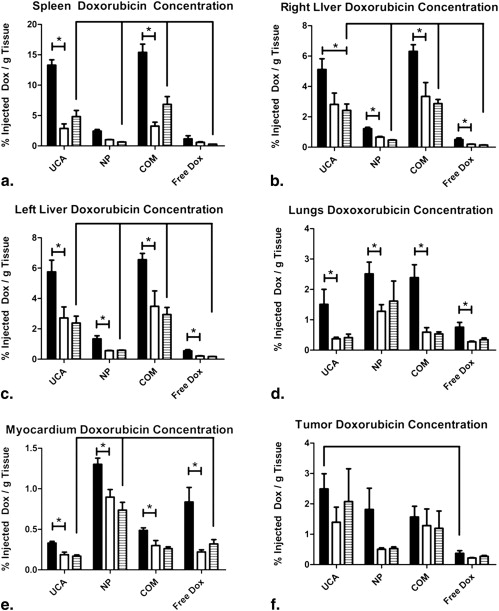
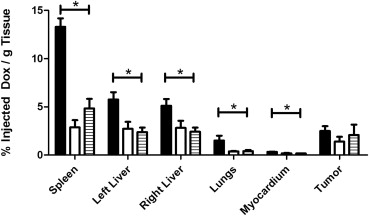
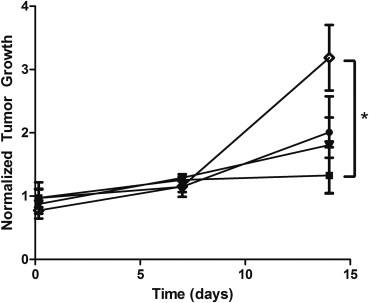
Animals treated with microbubbles had significantly lower plasma doxorubicin concentrations (0.466 ± 0.068%/mL) compared with free doxorubicin (3.033 ± 0.612%/mL, P = .0019). Drug levels in the myocardium were significantly lower in animals treated with microbubbles compared to free doxorubicin (0.168%/g tissue vs. 0.320%/g, P = .0088). Tumors treated with microbubbles showed significantly higher drug levels than tumors treated with free doxorubicin (2.491 ± 0.501 %/g vs. 0.373 ± 0.087 %/g, P = .0472). These tumors showed significantly less growth than tumors treated with free doxorubicin ( P = .0390).
Conclusions
Doxorubicin loaded microbubbles triggered with ultrasound provided enhanced, sustained drug delivery to tumors, reduced plasma and myocardium doxorubicin levels, and arresting tumor growth. The results suggest that in situ generation of nano particles provides a superior treatment over injection of free drug and also de novo synthesized nanoparticles.
The hyperpermeable vasculature of a tumor created during angiogenesis is characterized by pore sizes ranging from 380 to 780 nm, allowing nanoparticles (NP) to extravasate into the interstitium . Additionally, the tumor architecture generally lacks adequate lymphatic drainage, allowing these particles to accumulate over time .
Ultrasound contrast agents (UCA) are small (generally 1–6 μm) gas bubbles encapsulated within a stabilizing shell. When the agent is exposed to ultrasound, the gas core of the agent will expand and contract with a wall velocity on the order of hundreds of meters per second . These agents are generally restricted to circulation within the vascular system because of their size, but are small enough to penetrate into angiogenic vessels . When UCA are exposed to sufficient ultrasound intensity, the agents can cavitate and create enough shear force to rupture cell membranes and increase the permeability of the capillary wall, allowing particles to escape the vessel and penetrate tens of microns into the tumor interstitium . Vascular permeability can be enhanced through the use of UCA combined with targeted ultrasound .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Figure 1
Schematic of ultrasound triggered drug delivery. Doxorubicin loaded UCA pass freely through the vasculature until exposed to ultrasound where they experience 1) acoustic radiation forces that push the microbubbles to the vessel wall. The oscillating pressure wave will also lead to 2) microbubble cavitation as the gas core expands and contracts in response to changes in pressure. When exposed to sufficiently strong ultrasound pulses, the microbubble will undergo 3) inertial cavitation resulting in the destruction of the polymer shell, creating drug loaded polymer fragments less than 400 nm. The energy released in the process of microbubble destruction is sufficient to 4) enhance the permeability of the vessel wall. The fragments can then begin to 5) accumulate within the tumor interstitium, potentially, through acoustic radiation force and with time, circulating fragments will accumulate though the enhanced permeability and retention effect. Lodged polymer fragments can 6) slowly degrade providing a sustained localized release of the chemotherapeutic agent.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Materials
Get Radiology Tree app to read full this article<
Microbubble Fabrication
Get Radiology Tree app to read full this article<
Nanoparticle Fabrication
Get Radiology Tree app to read full this article<
Cell Culture
Get Radiology Tree app to read full this article<
Animals
Get Radiology Tree app to read full this article<
Tumor Implantation
Get Radiology Tree app to read full this article<
Treatments
Get Radiology Tree app to read full this article<
Plasma Doxorubicin Quantification
Get Radiology Tree app to read full this article<
Organ Doxorubicin Quantification
Get Radiology Tree app to read full this article<
Tumor Growth Measurements
Get Radiology Tree app to read full this article<
Histology and Autoradiography
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Plasma Doxorubicin Levels
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Organ and Tumor Doxorubicin Levels
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Tumor Growth
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Autoradiography and Histology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Actual Drug Levels Generated by Ultrasound Treatment of Drug-loaded Contrast Agent
Time Myocardium (ng/mg Tissue) Spleen (ng/mg Tissue) Left Liver (ng/mg Tissue) Right Liver (ng/mg Tissue) Lungs (ng/mg Tissue) Tumor (ng/mg Tissue) 4 hours 0.554 ± 0.035 22.272 ± 1.482 9.637 ± 1.297 8.577 ± 1.179 2.525 ± 0.832 4.174 ± 0.840 7 days 0.314 ± 0.052 4.815 ± 1.250 4.552 ± 1.213 4.718 ± 1.248 0.630 ± 0.081 2.340 ± 0.829 14 days 0.281 ± 0.028 8.099 ± 1.679 3.99 ± 0.767 4.061 ± 0.699 0.688 ± 0.199 3.478 ± 1.809
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Maeda H., Wu J., Sawa T., et. al.: Tumor vascular permeability and the EPR effect in macromolecular therapeutics: a review. J Control Release 2000; 65: pp. 271-284.
2. Hobbs S.K., Monsky W.L., Yuan F., et. al.: Regulation of transport pathways in tumor vessels: role of tumor type and microenvironment. Proc Natl Acad Sci U S A 1998; 95: pp. 4607-4612.
3. Vaupel P.: Tumor microenvironmental physiology and its implications for radiation oncology. Semin Radiat Oncol 2004; 14: pp. 198-206.
4. Ferrara K., Pollard R., Borden M.: Ultrasound microbubble contrast agents: fundamentals and application to gene and drug delivery. Annu Rev Biomed Eng 2007; 9: pp. 415-447.
5. Eisenbrey J.R., Forsberg F.: Contrast-enhanced ultrasound for molecular imaging of angiogenesis. Eur J Nucl Med Mol Imaging 2010; 37: pp. 138-146.
6. Ferrara K.W.: Driving delivery vehicles with ultrasound. Adv Drug Deliv Rev 2008; 60: pp. 1097-1102.
7. Bekeredjian R., Katus H.A., Kuecherer H.F.: Therapeutic use of ultrasound targeted microbubble destruction: a review of non-cardiac applications. Ultraschall Med 2006; 27: pp. 134-140.
8. Price R.J., Skyba D.M., Kaul S., et. al.: Delivery of colloidal particles and red blood cells to tissue through microvessel ruptures created by targeted microbubble destruction with ultrasound. Circulation 1998; 98: pp. 1264-1267.
9. Tinkov S., Winter G., Coester C., et. al.: New doxorubicin-loaded phospholipid microbubbles for targeted tumor therapy: part I—formulation development and in-vitro characterization. J Control Release 2010; 143: pp. 143-150.
10. Husseini G.A., Diaz de la Rosa M.A., Gabuji T., et. al.: Release of doxorubicin from unstabilized and stabilized micelles under the action of ultrasound. J Nanosci Nanotechnol 2007; 7: pp. 1028-1033.
11. Gao Z.-G., Fain H.D., Rapoport N.: Controlled and targeted tumor chemotherapy by micellar-encapsulated drug and ultrasound. J Control Release 2005; 102: pp. 203-222.
12. Kheirolomoom A., Dayton P.A., Lum A.F.H., et. al.: Acoustically-active microbubbles conjugated to liposomes: characterization of a proposed drug delivery vehicle. J Control Release 2007; 118: pp. 275-284.
13. Jones M., Leroux J.: Polymeric micelles—a new generation of colloidal drug carriers. Eur J Pharm Biopharm 1999; 48: pp. 101-111.
14. Alberts D.S., Garcia D.J.: Safety aspects of pegylated liposomal doxorubicin in patients with cancer. Drugs 1997; 54: pp. 30-35.
15. Kooiman K., Bohmer M.R., Emmer M., et. al.: Oil-filled polymer microcapsules for ultrasound-mediated delivery of lipophilic drugs. J Control Release 2009; 133: pp. 109-118.
16. Eisenbrey J.R., Burstein O.M., Kambhampati R., et. al.: Development and optimization of a doxorubicin loaded poly(lactic acid) contrast agent for ultrasound directed drug delivery. J Control Release 2010; 143: pp. 38-44.
17. El-Sherif D.M., Wheatley M.A.: Development of a novel method for synthesis of a polymeric ultrasound contrast agent. J Biomed Mater Res A 2003; 66: pp. 347-355.
18. Eisenbrey J.R., Huang P., Hsu J., et. al.: Ultrasound triggered cell death in vitro with doxorubicin loaded poly lactic-acid contrast agents. Ultrasonics 2009; 49: pp. 628-633.
19. Eisenbrey J.R., Soulen M.C., Wheatley M.A.: Delivery of encapsulated Doxorubicin by ultrasound-mediated size reduction of drug-loaded polymer contrast agents. IEEE Trans Biomed Eng 2010; 57: pp. 24-28.
20. Gewirtz D.A.: A critical evaluation of the mechanisms of action proposed for the antitumor effects of the anthracycline antibiotics adriamycin and daunorubicin. Biochem Pharmacol 1999; 57: pp. 727-741.
21. Singal P.K., Iliskovic N.: Doxorubicin-induced cardiomyopathy. N Engl J Med 1998; 339: pp. 900-905.
22. Gabizon A., Catane R., Uziely B., et. al.: Prolonged circulation time and enhanced accumulation in malignant exudates of doxorubicin encapsulated in polyethylene-glycol coated liposomes. Cancer Res 1994; 54: pp. 987-992.
23. Nishiyama N., Kataoka K.: Current state, achievements, and future prospects of polymeric micelles as nanocarriers for drug and gene delivery. Pharmacol Ther 2006; 112: pp. 630-648.
24. Brigger I., Dubernet C., Couvreur P.: Nanoparticles in cancer therapy and diagnosis. Adv Drug Deliv Rev 2002; 54: pp. 631-651.
25. Tewes F., Munnier E., Antoon B., et. al.: Comparative study of doxorubicin-loaded poly(lactide-co-glycolide) nanoparticles prepared by single and double emulsion methods. Eur J Pharm Biopharm 2007; 66: pp. 488-492.
26. Maataoui A., Qian J., Vossoughi D., et. al.: Transarterial chemoembolization alone and in combination with other therapies: a comparative study in an animal HCC model. Eur Radiol 2005; 15: pp. 127-133.
27. Yang R., Rescorla F.J., Reilly C.R., et. al.: A reproducible rat liver cancer model for experimental therapy: introducing a technique of intrahepatic tumor implantation. J Surg Res 1992; 52: pp. 193-198.
28. Lum A.F., Borden M.A., Dayton P.A., et. al.: Ultrasound radiation force enables targeted deposition of model drug carriers loaded on microbubbles. J Control Release 2006; 111: pp. 128-134.
29. Goldberg B.B., Liu J.B., Forsberg F.: Ultrasound contrast agents: a review. Ultrasound Med Biol 1994; 20: pp. 319-333.
30. Storm G., Belliot S.O., Daemen T., et. al.: Surface modification of nanoparticles to oppose uptake by the mononuclear phagocyte system. Adv Drug Deliv Rev 1995; 17: pp. 31-48.
31. Brannon-Peppas L., Blanchette J.O.: Nanoparticle and targeted systems for cancer therapy. Adv Drug Deliv Rev 2004; 56: pp. 1649-1659.
32. Rahman A., Ganjei A., Neefe J.R.: Comparative immunotoxicity of free doxorubicin and doxorubicin encapsulated in cardiolipin liposomes. Cancer Chemother Pharmacol 1986; 16: pp. 28-34.
33. Minotti G., Menna P., Salvatorelli E., et. al.: Anthracyclines: molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharmacol Rev 2004; 56: pp. 185-229.
34. Namur J., Wassef M., Millot J.-M., et. al.: Drug-eluting beads for liver embolization: concentration of doxorubicin in tissue and in beads in a pig model. J Vasc Interv Radiol 2010; 21: pp. 259-267.
35. Le Bot M.A., Begue J.M., Kernaleguen D., et. al.: Different cytotoxicity and metabolism of doxorubicin, daunorubicin, epirubicin, esorubicin and idarubicin in cultured human and rat hepatocytes. Biochem Pharmacol 1988; 37: pp. 3877-3887.
36. Yuan S., Zhang X., Lu L., et. al.: Anticancer activity of methoxymorpholinyl doxorubicin (PNU 152243) on human hepatocellular carcinoma. Anticancer Drugs 2004; 15: pp. 641-646.
37. Chuu J.J., Liu J.M., Tsou M.H., et. al.: Effects of paclitaxel and doxorubicin in histocultures of hepatocellular carcinomas. J Biomed Sci 2007; 14: pp. 233-244.
38. Schlosser T., Pohl C., Veltmann C., et. al.: Feasibility of the flash-replenishment concept in renal tissue: which parameters affect the assessment of the contrast replenishment?. Ultrasound Med Biol 2001; 27: pp. 937-944.
39. Shortencarier M.J., Dayton P.A., Bloch S.H., et. al.: A method for radiation-force localized drug delivery using gas-filled lipospheres. IEEE Trans Ultrason Ferroelectrics Frequency Control 2004; 51: pp. 222-831.