
Rationale and Objectives
The purpose of this study was to measure the effect of distractions, in the form of telephone call interruptions, on radiology resident diagnostic accuracy.
Materials and Methods
Radiology resident discrepancy reports and reading room telephone logs at an academic tertiary care pediatric hospital were collected over a 13-month period. Phone call times and durations were recorded. Major discrepancy shifts (defined as a call shift where at least one major discrepancy was discovered the following morning by the attending radiologist between the resident preliminary and attending final reports), and dictation time stamps for each discrepant preliminary dictation were also recorded. Telephone call volume and preliminary report time stamps were compared between “discrepancy shifts” and “no discrepancy shifts.”
Results
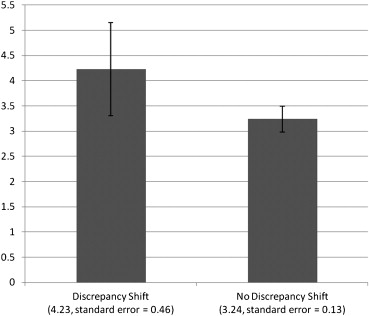
Each call shift spanned 14 hours, during which one radiology resident was responsible for the generation of preliminary interpretations. Review of the discrepancy log data revealed 51 major discrepancies in 41 shifts, of which 39 discrepancies had documented error details and resident preliminary report time stamps. The average number of telephone calls for the “discrepancy shifts” was slightly greater than the “no discrepancy shifts” (48.59 vs. 44.02) but was not statistically significant ( P = .0575). However, there was a statistically significant increase in the average number of phone calls in the 1 hour preceding the generation of a discrepant preliminary report versus the “no discrepancy shifts” (4.23 vs. 3.24 calls, P = .027). One additional phone call during the hour preceding the generation of a discrepant preliminary report resulted in a 12% increased likelihood of a resident error ( P = .017).
Conclusions
Distractions in the form of telephone call interruptions may negatively impact on-call radiology resident diagnostic accuracy. Efforts should be made to limit distractions in the reading room.
At many academic institutions, diagnostic radiology residents are often the sole practitioner responsible for after-hour radiology coverage, generating preliminary interpretations of examinations that are later reviewed and finalized by the attending radiologist. Radiology resident on-call responsibilities often require the ability to multitask, toggling between medical functions (interpreting examinations, interacting with consulting physicians and technologists, and consenting patients) and nonmedical functions (answering telephone calls and returning pages). The shifting of focus between multiple tasks has the potential to alter the resident’s mind-set with the potential for the introduction of medical errors.
Research and experience in complex “knowledge-intensive service environments” have shown that interruptions in workflow create inefficiencies, introduce barriers to productivity, and can contribute to errors . This is also true of the medical environment, a highly complex, cognitive-rich, service environment, with a great deal of attention and effort directed toward patient safety initiatives and health care system accountability . Prior research has linked interruptions with errors in the laboratory setting and clinical setting and the effect of interruptions on patient safety and workplace stress .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
![Figure 1, An 11-year-old boy with hand trauma and suspected fracture. There is a subtle cortical buckle of the proximal metaphysis of the proximal third phalanx ( a , white arrow ), seen best on the magnified image of the same study (magnified at the workstation [ b , white arrow ]) consistent with a Salter–Harris type II fracture. This fracture was not prospectively identified by the radiology resident.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/DoTelephoneCallInterruptionsHaveanImpactonRadiologyResidentDiagnosticAccuracy/0_1s20S1076633214003079.jpg)
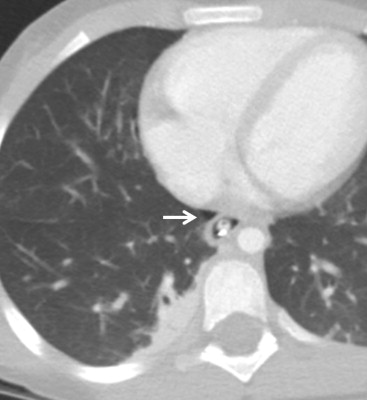
Table 1
Discrepancies by Imaging Modality and Body Region
Imaging Modality Chest Abdomen Extremity Genitourinary Tract Spine Pelvis Total Film 13 7 7 0 1 0 28 Computed tomography 3 2 1 0 1 1 8 Ultrasound 0 0 0 3 0 0 3 Total 16 9 8 3 2 1 39
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Froehle C.M., White D.L.: Interruption and forgetting in knowledge-intensive service environments. Prod Oper Manag 2013; 23: pp. 704-722.
2. Kohn L.T.Corrigan J.Donaldson M.S.To err is human: building a safer health system.2000.National Academy PressWashington, District of Columbia:
3. Stelfox H.T., Palmisani S., Scurlock C., et. al.: The “To Err is Human” report and the patient safety literature. Qual Safety Health Care 2006; 15: pp. 174-178.
4. Sittig D.F., Singh H.: Electronic health records and national patient-safety goals. N Engl J Med 2012; 367: pp. 1854-1860.
5. Radecki R.P., Sittig D.F.: Application of electronic health records to the Joint Commission’s 2011 National Patient Safety Goals. JAMA 2011; 306: pp. 92-93.
6. Blendon R.J., DesRoches C.M., Brodie M., et. al.: Views of practicing physicians and the public on medical errors. N Engl J Med 2002; 347: pp. 1933-1940.
7. Einstein G.O., McDaniel M.A., Williford C.L., et. al.: Forgetting of intentions in demanding situations is rapid. J Exp Psychol Appl 2003; 9: pp. 147-162.
8. Eyrolle H., Cellier J.M.: The effects of interruptions in work activity: field and laboratory results. Appl Ergon 2000; 31: pp. 537-543.
9. Meeks D.W., Takian A., Sittig D.F., et. al.: Exploring the sociotechnical intersection of patient safety and electronic health record implementation. J Am Med Inform Assoc 2014; 21: pp. e28-e34.
10. Joint Commission Center for Transforming Healthcare, SCHA collaborate on high-reliability program. Bull Am Coll Surg 2013; 98: pp. 65.
11. McGillis Hall L., Pedersen C., Fairley L.: Losing the moment: understanding interruptions to nurses’ work. J Nurs Adm 2010; 40: pp. 169-176.
12. Sorensen E.E., Brahe L.: Interruptions in clinical nursing practice. J Clin Nur 2013; 23: pp. 1274-1282.
13. Hall L.M., Ferguson-Pare M., Peter E., et. al.: Going blank: factors contributing to interruptions to nurses’ work and related outcomes. J Nurs Manag 2010; 18: pp. 1040-1047.
14. Arora S., Hull L., Sevdalis N., et. al.: Factors compromising safety in surgery: stressful events in the operating room. Am J Surg 2010; 199: pp. 60-65.
15. Yu J.P., Kansagra A.P., Mongan J.: The radiologist’s workflow environment: evaluation of disruptors and potential implications. J Am Coll Radiol 2014; 11: pp. 589-593.
16. Levin D.C., Rao J.M., Parker L., et. al.: Analysis of radiologists’ imaging workload trends by place of service. J Am Coll Radiol 2013; 10: pp. 760-763.
17. Rosenstein A.H., Mudge-Riley M.: The impact of stress and burnout on physician satisfaction and behaviors. Physician Exec 2010; 36: pp. 16-18. 20, 22-3
18. Holt G.R.: Physician burnout: a serious concern for the medical profession. South Med J 2013; 106: pp. 297.
19. Shanafelt T., Dyrbye L.: Oncologist burnout: causes, consequences, and responses. J Clin Oncol 2012; 30: pp. 1235-1241.
20. Dhanoa D., Dhesi T.S., Burton K.R., et. al.: The evolving role of the radiologist: the Vancouver workload utilization evaluation study. J Am Coll Radiol 2013; 10: pp. 764-769.
21. Cooper V.F., Goodhartz L.A., Nemcek A.A., et. al.: Radiology resident interpretations of on-call imaging studies: the incidence of major discrepancies. Acad Radiol 2008; 15: pp. 1198-1204.
22. Flink C.C., Mueller J.S., Kiproff P.M.: Impact of resident call eligibility on major discrepancy rate. Acad Radiol 2010; 17: pp. 1299-1301.
23. Maloney E., Lomasney L.M., Schomer L.: Application of the RADPEER scoring language to interpretation discrepancies between diagnostic radiology residents and faculty radiologists. J Am Coll Radiol 2012; 9: pp. 264-269.
24. Miyakoshi A., Nguyen Q.T., Cohen W.A., et. al.: Accuracy of preliminary interpretation of neurologic CT examinations by on-call radiology residents and assessment of patient outcomes at a level I trauma center. J Am Coll Radiol 2009; 6: pp. 864-870.
25. Ruchman R.B., Jaeger J., Wiggins E.F., et. al.: Preliminary radiology resident interpretations versus final attending radiologist interpretations and the impact on patient care in a community hospital. AJR Am J Roentgenol 2007; 189: pp. 523-526.
26. Ruma J., Klein K.A., Chong S., et. al.: Cross-sectional examination interpretation discrepancies between on-call diagnostic radiology residents and subspecialty faculty radiologists: analysis by imaging modality and subspecialty. J Am Coll Radiol 2011; 8: pp. 409-414.
27. Shah N.A., Hoch M., Willis A., et. al.: Correlation among on-call resident study volume, discrepancy rate, and turnaround time. Acad Radiol 2010; 17: pp. 1190-1194.
28. Walls J., Hunter N., Brasher P.M., et. al.: The DePICTORS study: discrepancies in preliminary interpretation of CT scans between on-call residents and staff. Emerg Radiol 2009; 16: pp. 303-308.
29. Altmann E.M., Trafton J.G., Hambrick D.Z.: Momentary interruptions can derail the train of thought. J Exp Psychol Gen 2014; 143: pp. 215-226.
30. “The Biggest Office Interruptions Are…” Available at: http://online.wsj.com/news/articles/SB10001424127887324123004579057212505053076 . Accessed December 18, 2013.
31. Lindsay R., McKinstry S., Vallely S., et. al.: What influences clinician’s satisfaction with radiology services?. Insights Imaging 2011; 2: pp. 425-430.