
Rationale and Objectives
To prospectively evaluate the influence of the clinical pretest probability assessed by the Morise score onto image quality and diagnostic accuracy in coronary dual-source computed tomography angiography (DSCTA).
Materials and Methods
In 61 patients, DSCTA and invasive coronary angiography were performed. Subjective image quality and accuracy for stenosis detection (>50%) of DSCTA with invasive coronary angiography as gold standard were evaluated. The influence of pretest probability onto image quality and accuracy was assessed by logistic regression and chi-square testing. Correlations of image quality and accuracy with the Morise score were determined using linear regression.
Results
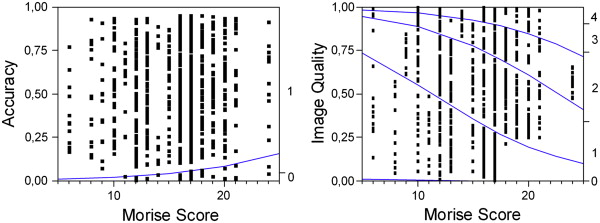
Thirty-eight patients were categorized into the high, 21 into the intermediate, and 2 into the low probability group. Accuracies for the detection of significant stenoses were 0.94, 0.97, and 1.00, respectively. Logistic regressions and chi-square tests showed statistically significant correlations between Morise score and image quality ( P < .0001 and P < .001) and accuracy ( P = .0049 and P = .027). Linear regression revealed a cutoff Morise score for a good image quality of 16 and a cutoff for a barely diagnostic image quality beyond the upper Morise scale.
Conclusion
Pretest probability is a weak predictor of image quality and diagnostic accuracy in coronary DSCTA. A sufficient image quality for diagnostic images can be reached with all pretest probabilities. Therefore, coronary DSCTA might be suitable also for patients with a high pretest probability.
Coronary computed tomography angiography (CTA) has evolved as a tool to noninvasively assess coronary artery disease (CAD). Several recent studies have shown the potential of 64-slice and dual-source CT (DSCT) to image the coronary tree and to detect and grade stenoses . Although excellent results have been reported for patients with low and intermediate pretest probabilities , it is known that the image quality of CTA may suffer in patients with a higher pretest probability because of obesity, blooming artifacts caused by calcified plaques, or irregular heart rates . A large study of 64-slice CTA performed by Meijboom et al has shown that this modality is severely limited in patients with a high pretest probability . DSCT with its high temporal resolution and x-ray output has the potential to improve image quality in patients with high pretest probabilities . All previous studies investigating the accuracy of coronary DSCT angiography (DSCTA) known to the authors have focused on certain patient collectives with a homogenous distribution of pretest probabilities or have not evaluated the impact of different pretest probabilities onto the diagnostic accuracy of coronary DSCTA. Furthermore, the results of these studies are hardly comparable because the pretest probability was not defined unequivocally in all studies. Therefore, in this study, the image quality and accuracy of coronary DSCTA in a heterogeneous patient collective is assessed with regards to the patients’ pretest probability.
Materials and methods
Patients and Morise Score
The local ethics committee agreed to this study. Between April 2007 and November 2007, 61 consecutive patients (42 males, mean age 63 ± 10 years) who were referred for invasive coronary angiography (ICA) because of suspected CAD were included into the study and received additional coronary DSCTA 1 day before ICA. All CT examinations were performed at the same institution (a large university hospital). All patients gave their informed consent to participate in this study. Exclusion criteria were known previous myocardial infarction, known CAD, allergic reaction to iodinated contrast media, impaired renal function, hyperthyroidism (basal thyroid-stimulating hormone <0.03 μL/L in combination with elevation of the peripheral thyroid hormones), pregnancy, and unstable clinical conditions.
Get Radiology Tree app to read full this article<
Table 1
Factors for the Calculation of the Morise Score
Points Condition Age 3 <40 (male), <50 (female) 6 40–55 (male) 50–64 (female) 9 >55 (male), >65 (female) Estrogen −3 Estrogen positive 0 Male/unknown 3 Estrogen negative Symptoms 0 Non-anginal 3 Atypical angina 5 Typical angina Hypertension 1 If positive Smoking 1 If positive Hyperlipidemia 1 If positive Family history 1 If positive Obesity 1 If positive Diabetes 2 If positive
Get Radiology Tree app to read full this article<
DSCT
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ICA
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Quality and Accuracy
Get Radiology Tree app to read full this article<
Table 2
Numbers and Percentages of Segments of every Image Quality Score Point in each Pretest Probability Group
Image quality score 1 2 3 4 Pretest probability (#) (%) (#) (%) (#) (%) (#) (%) Low (n = 26) 22 84.6 1 3.8 2 7.7 1 3.8 Medium (n = 273) 99 36.2 122 44.7 39 14.3 13 4.8 High (n = 494) 154 31.2 200 40.5 89 18.0 51 10.3 All (n = 793) 275 34.7 323 40.7 130 16.4 65 8.2
Image quality score: 1: excellent, 2: good, 3: barely diagnostic, 4: insufficient.
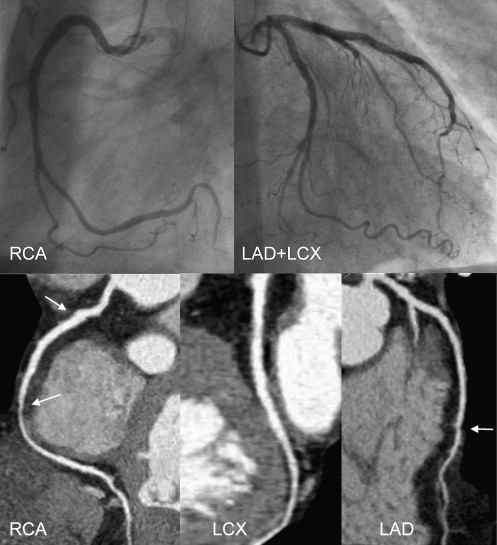
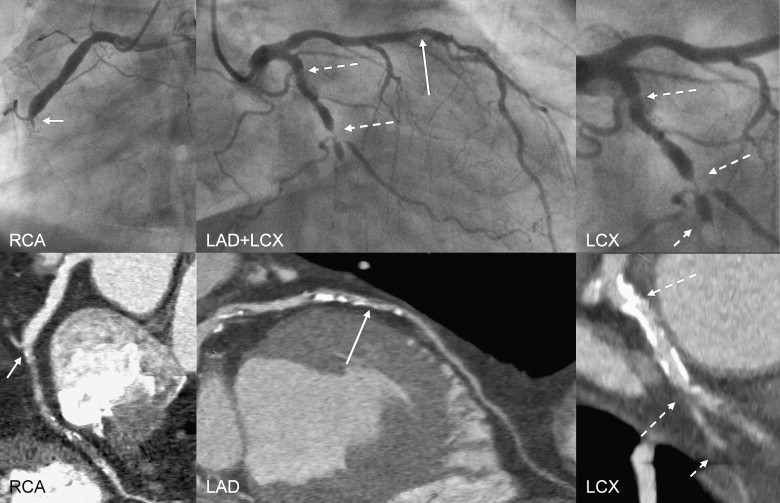
Table 3
Results of DSCTA with ICA as Gold Standard in every Pretest Probability Group, Calculated Per patient and Per segment
Per patient Per segment Pretest probability TP TN FP FN TP TN FP FN Accuracy Low (n = 2) 0 2 (100%) 0 0 0 26 (100%) 0 0 1.00 Medium (n = 21) 5 (24%) 14 (67%) 2 (10%) 0 (0%) 17 (6%) 247 (90%) 7 (3%) 2 (1%) 0.97 High (n = 38) 18 (47%) 15 (39%) 4 (11%) 1 (3%) 63 (13%) 403 (82%) 25 (5%) 3 (1%) 0.94 All (n = 61) 23 (38%) 31 (51%) 6 (10%) 1 (2%) 80 (10%) 676 (85%) 32 (4%) 5 (1%) 0.95
TP, true positive; TN, true negative; TP, false positive; FN, false negative.
Table 4
Sensitivities, Specificities, Positive Predictive Values (PPV), and Negative Predictive Values (NPV) Given for each Pretest Probability Group and for the Whole
Per patient Per segment Pretest probability Sensitivity (%) Specificity (%) PPV
(%) NPV
(%) Sensitivity (%) Specificity (%) PPV
(%) NPV
(%) Low ND 100.0 ND 100.0 ND 100.0 ND 100.0 Medium 100.0 87.5 71.4 100.0 89.5 97.2 70.8 99.2 High 94.7 78.9 81.8 93.8 95.5 94.2 71.6 99.3 All 95.8 83.8 79.3 96.9 94.1 95.5 71.4 99.3
ND, not defined.
Collective calculated per patient and per segment.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Schoepf U.J., Zwerner P.L., Savino G., et. al.: Coronary CT angiography. Radiology 2007; 244: pp. 48-63.
2. Achenbach S.: Developments in coronary CT angiography. Curr Cardiol Rep 2008; 10: pp. 51-59.
3. Hoffmann M.H., Shi H., Schmitz B.L., et. al.: Noninvasive coronary angiography with multislice computed tomography. JAMA 2005; 293: pp. 2471-2478.
4. Muhlenbruch G., Seyfarth T., Soo C.S., et. al.: Diagnostic value of 64-slice multi-detector row cardiac CTA in symptomatic patients. Eur Radiol 2007; 17: pp. 603-609.
5. Ravipati G., Aronow W.S., Lai H., et. al.: Comparison of sensitivity, specificity, positive predictive value, and negative predictive value of stress testing versus 64-multislice coronary computed tomography angiography in predicting obstructive coronary artery disease diagnosed by coronary angiography. Am J Cardiol 2008; 101: pp. 774-775.
6. Choi E.K., Choi S.I., Rivera J.J., et. al.: Coronary computed tomography angiography as a screening tool for the detection of occult coronary artery disease in asymptomatic individuals. J Am Coll Cardiol 2008; 52: pp. 357-365.
7. Schlosser T., Mohrs O.K., Magedanz A., et. al.: Noninvasive coronary angiography using 64-detector-row computed tomography in patients with a low to moderate pretest probability of significant coronary artery disease. Acta Radiol 2007; 48: pp. 300-307.
8. Brodoefel H., Tsiflikas I., Burgstahler C., et. al.: Cardiac dual-source computed tomography: effect of body mass index on image quality and diagnostic accuracy. Invest Radiol 2008; 43: pp. 712-718.
9. Shapiro M.D., Pena A.J., Nichols J.H., et. al.: Efficacy of pre-scan beta-blockade and impact of heart rate on image quality in patients undergoing coronary multidetector computed tomography angiography. Eur J Radiol 2008; 66: pp. 37-41.
10. Meijboom W.B., van Mieghem C.A., Mollet N.R., et. al.: 64-slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol 2007; 50: pp. 1469-1475.
11. Chinnaiyan K.M., McCullough P.A., Flohr T.G., et. al.: Improved noninvasive coronary angiography in morbidly obese patients with dual-source computed tomography. J Cardiovasc Comput Tomogr 2009; 3: pp. 35-42.
12. Rixe J., Rolf A., Conradi G., et. al.: Detection of relevant coronary artery disease using dual-source computed tomography in a high probability patient series: comparison with invasive angiography. Circ J 2009; 73: pp. 316-322.
13. Alkadhi H., Scheffel H., Desbiolles L., et. al.: Dual-source computed tomography coronary angiography: influence of obesity, calcium load, and heart rate on diagnostic accuracy. Eur Heart J 2008; 29: pp. 766-776.
14. Ropers U., Ropers D., Pflederer T., et. al.: Influence of heart rate on the diagnostic accuracy of dual-source computed tomography coronary angiography. J Am Coll Cardiol 2007; 50: pp. 2393-2398.
15. Weustink A.C., Meijboom W.B., Mollet N.R., et. al.: Reliable high-speed coronary computed tomography in symptomatic patients. J Am Coll Cardiol 2007; 50: pp. 786-794.
16. Burgstahler C., Reimann A., Brodoefel H., et. al.: Quantitative parameters to compare image quality of non-invasive coronary angiography with 16-slice, 64-slice and dual-source computed tomography. Eur Radiol 2009; 19: pp. 584-590.
17. Morise A., Evans M., Jalisi F., et. al.: A pretest prognostic score to assess patients undergoing exercise or pharmacological stress testing. Heart 2007; 93: pp. 200-204.
18. Morise A.P., Jalisi F.: Evaluation of pretest and exercise test scores to assess all-cause mortality in unselected patients presenting for exercise testing with symptoms of suspected coronary artery disease. J Am Coll Cardiol 2003; 42: pp. 842-850.
19. Kuettner A., Beck T., Drosch T., et. al.: Diagnostic accuracy of noninvasive coronary imaging using 16-detector slice spiral computed tomography with 188 ms temporal resolution. J Am Coll Cardiol 2005; 45: pp. 123-127.
20. Leber A.W., Johnson T., Becker A., et. al.: Diagnostic accuracy of dual-source multi-slice CT-coronary angiography in patients with an intermediate pretest likelihood for coronary artery disease. Eur Heart J 2007; 28: pp. 2354-2360.
21. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
22. Johnson T.R., Nikolaou K., Busch S., et. al.: Diagnostic accuracy of dual-source computed tomography in the diagnosis of coronary artery disease. Invest Radiol 2007; 42: pp. 684-691.
23. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
24. Ong T.K., Chin S.P., Liew C.K., et. al.: Accuracy of 64-row multidetector computed tomography in detecting coronary artery disease in 134 symptomatic patients: influence of calcification. Am Heart J 2006; 151: pp. 1323. e1321–1326
25. Schroeder S., Achenbach S., Bengel F., et. al.: Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J 2008; 29: pp. 531-556.
26. Scheffel H., Alkadhi H., Plass A., et. al.: Accuracy of dual-source CT coronary angiography: first experience in a high pre-test probability population without heart rate control. Eur Radiol 2006; 16: pp. 2739-2747.