
Rationale and Objective
The objective of this study was to evaluate whether quantitative enhancement or perfusion measurements on preprocedure triphasic computed tomography (CT) can be used to predict response or overall survival after embolization of hepatocellular carcinoma.
Materials and Methods
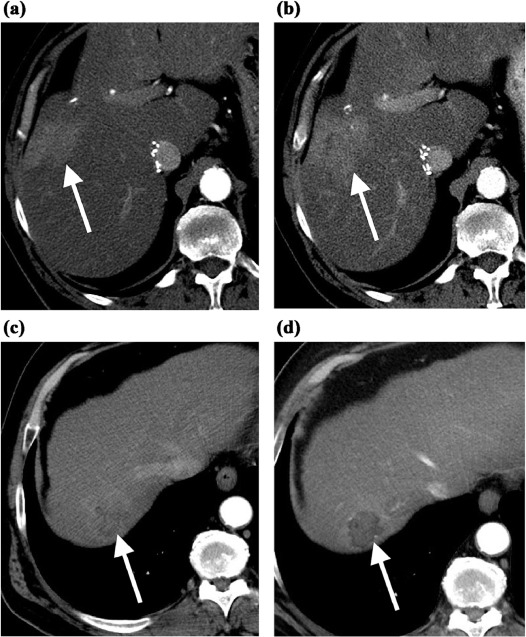
The institutional review board approved this retrospective review of 63 patients with hepatocellular carcinoma treated with particle embolization between March 2009 and December 2014. Quantitative enhancement and perfusion measurements were performed on the target tumor and the background liver on the triphasic CT performed before treatment. Microvascular invasion (MVI) and degree of differentiation were determined from a core biopsy specimen. Quantitative enhancement and perfusion values were then correlated with pathology (two-tailed t test), response to embolization on modified Response Evaluation Criteria In Solid Tumors (two-tailed t test), and overall survival after embolization (Cox proportional hazards model).
Results
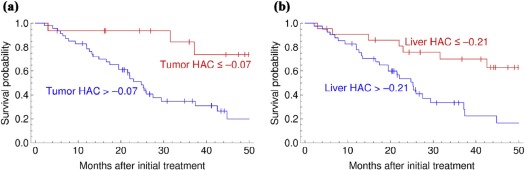
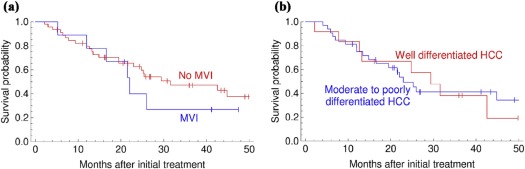
Arterial enhancement did not predict immediate response or overall survival after embolization. The degree of differentiation or presence of MVI also did not predict immediate response or overall survival after embolization. However, high hepatic artery coefficient or low portal vein coefficient, both in the tumor ( P = .011 and P = .004) and in the background liver ( P = .015 and P = .009), were associated with worse survival. Hepatic artery coefficient, both in the tumor ( P = .025) and in the background liver ( P = .013), were independent predictors of survival in a multivariate model including the Child-Pugh score and the BCLC stage.
Conclusions
Tumor and liver perfusion parameters estimated from preprocedure triphasic CT were predictive of survival after embolization. Arterial-phase enhancement and histology (degree of differentiation or MVI) did not predict immediate response or overall survival after particle embolization.
Introduction
Treatment options for unresectable and unablatable hepatocellular carcinoma (HCC) include transarterial embolization (TAE), transarterial chemoembolization (TACE) using either lipiodol or drug-eluting beads, radioembolization, and sorafenib. Recent randomized trials have shown no difference in overall survival for these treatment options, although there are differences in response rates and quality of life .
Regardless of the treatment, there are a subset of patients who do not respond . Although overall survival after the various different treatment options for unresectable HCC appears to be similar, there might be subgroups that do better with one treatment compared to another . Predicting which patients will have poor outcomes with one treatment option could potentially allow these patients to be directed to a different treatment option.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Patient Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Transarterial Embolization
Get Radiology Tree app to read full this article<
Imaging Protocol
Get Radiology Tree app to read full this article<
Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
TABLE 1
Patient Characteristics
n (%) Child-Pugh score A 58 (92) B 5 (8) C 0 (0) BCLC stage 0 1 (1) A 18 (29) B 34 (54) C 10 (16) Etiology of liver disease HBV 10 (16) HCV 18 (29) Alcoholism 6 (10) NASH 5 (8) Other 18 (29) Multiple 5 (8) Cirrhosis Yes 37 (59) No 26 (41) Pathology (degree of differentiation) Well differentiated 12 (19) Moderately differentiated 26 (41) Poorly differentiated 6 (10) Undifferentiated 0 (0) Fibrolamellar 2 (3) Not specified 8 (13) Core biopsy not performed 9 (14) Pathology (MVI) Yes 9 (14) No 45 (71) Core biopsy not performed 9 (14)
BCLC, Barcelona Clinic Liver Cancer; HBV, hepatitis B virus; HCV, hepatitis C virus; MVI, microvascular invasion; NASH, nonalcoholic steatohepatitis.
Get Radiology Tree app to read full this article<
Predicting Response to Embolization
Get Radiology Tree app to read full this article<
TABLE 2
Hepatocellular Carcinoma Enhancement, Perfusion Parameters, and Pathology Did Not Predict CR After Embolization
CR (Av. ± SD) Non-CR (Av. ± SD)P Value HAC 0.03 ± 0.22 0.08 ± 0.29 .45 PVC 0.44 ± 0.27 0.31 ± 0.41 .14 AEF 0.74 ± 0.25 0.94 ± 0.83 .21 Arterial-phase enhancement (HU) 44 ± 17 45 ± 36 .86 Portal venous-phase enhancement (HU) 60 ± 15 53 ± 20 .13 Moderate to poorly differentiated 12/16 20/28 1.0 MVI 5/25 4/29 .72
AEF, arterial enhancement fraction; Av., average; CR, complete response; HAC, hepatic artery coefficient; MVI, microvascular invasion; PVC, portal vein coefficient; SD, standard deviation.
Get Radiology Tree app to read full this article<
Predicting Overall Survival After Embolization
Get Radiology Tree app to read full this article<
TABLE 3
Predictors of Overall Survival After Embolization of Hepatocellular Carcinoma (Cox Proportional Hazards Model)
Univariate Model
Relative Risk ( P Value) Multivariate Model
Relative Risk ( P Value) Tumor HAC 3.85 (.011 \* ) 4.38 (.025 \* ) PVC 0.32 (.004 \* ) AEF 1.39 (.115) Arterial-phase enhancement (HU) 1 (.73) PV-phase enhancement (HU) 0.99 (.28) Liver HAC 1.27 (.015 \* ) 1.33 (.013 \* ) PVC 0.75 (.009 \* ) Child-Pugh score 1.04 (.83) 1.08 (.684) BCLC stage 0 or A 0.69 (.34) 1 (n/a) B 0.55 (.084) 0.86 (.725) C 6.77 (2.9 × 10 −6 \* ) 6.31 (.00016 \* )
AEF, arterial enhancement fraction; BCLC, Barcelona Clinic Liver Cancer; HAC, hepatic artery coefficient; n/a, not applicable; PV, portal venous; PVC, portal vein coefficient.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Predicting Pathology From Imaging
Get Radiology Tree app to read full this article<
TABLE 4
Higher Arterial or Portal Venous-phase Enhancement Predicts Moderate to Poorly Differentiated Hepatocellular Carcinoma
Well-differentiated (Av. ± SD) Moderately to Poorly Differentiated (Av. ± SD)P Value Arterial-phase enhancement (HU) 29 ± 16 52 ± 52 .004 \* PV-phase enhancement (HU) 43 ± 19 58 ± 58 .028 \* HAC 0.02 ± 0.19 0.10 ± 0.10 .345 PVC 0.27 ± 0.34 0.37 ± 0.37 .415 AEF 0.94 ± 0.99 0.91 ± 0.91 .922
AEF, arterial enhancement fraction; Av., average; HAC, hepatic artery coefficient; PV, portal venous; PVC, portal vein coefficient; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Appendix S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Salem R., Gordon A.C., Mouli S., et. al.: Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology 2016; 151: pp. 1155-1163. e2
2. Vilgrain V., Bouattour M., Sibert A., et. al.: SARAH: A randomised controlled trial comparing efficacy and safety of selective internal radiation therapy (with yttrium-90 microspheres) and sorafenib in patients with locally advanced hepatocellular carcinoma. J Hepatol 2017; 66: pp. S85-S86.
3. Brown K.T., Do R.K., Gonen M., et. al.: Randomized trial of hepatic artery embolization for hepatocellular carcinoma using doxorubicin-eluting microspheres compared with embolization with microspheres alone. J Clin Oncol 2016; 34: pp. 2046-2053.
4. Biederman D.M., Titano J.J., Tabori N.E., et. al.: Outcomes of radioembolization in the treatment of hepatocellular carcinoma with portal vein invasion: resin versus glass microspheres. J Vasc Interv Radiol 2016; 27: pp. 812-821. e2
5. Katyal S., Oliver J.H., Peterson M.S., et. al.: Prognostic significance of arterial phase CT for prediction of response to transcatheter arterial chemoembolization in unresectable hepatocellular carcinoma: a retrospective analysis. AJR Am J Roentgenol 2000; 175: pp. 1665-1672.
6. Hu H.T., Kim J.H., Lee L.S., et. al.: Chemoembolization for hepatocellular carcinoma: multivariate analysis of predicting factors for tumor response and survival in a 362-patient cohort. J Vasc Interv Radiol 2011; 22: pp. 917-923.
7. Artinyan A., Nelson R., Soriano P., et. al.: Treatment response to transcatheter arterial embolization and chemoembolization in primary and metastatic tumors of the liver. HPB (Oxford) 2008; 10: pp. 396-404.
8. Kwan S.W., Fidelman N., Ma E., et. al.: Imaging predictors of the response to transarterial chemoembolization in patients with hepatocellular carcinoma: a radiological-pathological correlation. Liver Transpl 2012; 18: pp. 727-736.
9. Sato K.T., Omary R.A., Takehana C., et. al.: The role of tumor vascularity in predicting survival after yttrium-90 radioembolization for liver metastases. J Vasc Interv Radiol 2009; 20: pp. 1564-1569.
10. Boas F.E., Brody L.A., Erinjeri J.P., et. al.: Quantitative measurements of enhancement on preprocedure triphasic CT can predict response of colorectal liver metastases to radioembolization. AJR Am J Roentgenol 2016; 207: pp. 671-675.
11. Boas F.E., Kamaya A., Do B., et. al.: Classification of hypervascular liver lesions based on hepatic artery and portal vein blood supply coefficients calculated from triphasic CT scans. J Digit Imaging 2015; 28: pp. 213-223.
12. Lencioni R., Llovet J.M.: Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis 2010; 30: pp. 52-60.
13. Brown K.T.: Bland embolization for hepatic malignancies.Mauro M.A.Murphy K.P.J.Thomson K.R. et. al.Image-guided interventions.2014.ElsevierPhiladelphia, PA:pp. 467-475.
14. Budczies J., Klauschen F., Sinn B.V., et. al.: Cutoff Finder: a comprehensive and straightforward Web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012; 7: e51862
15. Herber S., Biesterfeld S., Franz U., et. al.: Correlation of multislice CT and histomorphology in HCC following TACE: predictors of outcome. Cardiovasc Intervent Radiol 2008; 31: pp. 768-777.
16. Lim K.C., Chow P.K., Allen J.C., et. al.: Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Ann Surg 2011; 254: pp. 108-113.
17. Jonas S., Bechstein W.O., Steinmuller T., et. al.: Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001; 33: pp. 1080-1086.
18. Lee E.C., Kim S.H., Park H., et. al.: Survival analysis after liver resection for hepatocellular carcinoma: a consecutive cohort of 1002 patients. J Gastroenterol Hepatol 2017; 32: pp. 1055-1063.
19. Choi J.Y., Lee J.M., Sirlin C.B.: CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology 2014; 272: pp. 635-654.
20. Kitao A., Zen Y., Matsui O., et. al.: Hepatocarcinogenesis: multistep changes of drainage vessels at CT during arterial portography and hepatic arteriography—radiologic-pathologic correlation. Radiology 2009; 252: pp. 605-614.
21. Gulberg V., Haag K., Rossle M., et. al.: Hepatic arterial buffer response in patients with advanced cirrhosis. Hepatology 2002; 35: pp. 630-634.