
Rationale and Objectives
To evaluate the performance of hybrid iterative reconstruction technique (h-IRT) on image quality (IQ) in abdominal dose-modified (DM) scans in phantom and in patients in comparison to filtered back projection (FBP).
Materials and Methods
An anthropomorphic phantom was scanned using various kVp (80–140) and mAs (25–100) settings. Images were reconstructed with FBP and h-IRT levels (1–6). In 69 adults (59.6 ± 13.54 years; 20 male, 49 female), DM computed tomography (CT) scans were performed using 120 kVp and 100–120 mAs. In 25/69, 5-mm FBP and h-IRT (levels 1–4 and 5) images were analyzed to validate IQ. The subsequent 44/69 had FBP and h-IRT (level 4) images reconstructed. Two readers evaluated 188 image series for IQ, noise, and artifacts. Objective and subjective data were analyzed using t -test and Wilcoxon signed-rank test, respectively. In 46/69 patients, prior dose CT was available for dose comparison.
Results
In the phantom, noise reduction ranged from 12% (h-IRT level 1) to 50% (level 6). In patients, h-IRT level 4 images were rated diagnostic in 69/69 exams but DM-FBP images were found nondiagnostic in 20/69 patients. The size-specific dose estimate (SSDE) was reduced by 55% in the dose-modified CT group, (SSDE:4.55 ± 1.15 mGy) over the prior dose protocol (SSDE:10.21 ± 3.5 mGy, P < .0001).
Conclusion
h-IRT improved IQ in abdominal DM-CT scans in phantom and in patients. Dose improvements were greater in smaller patients than larger ones.
Since the introduction of CT scanners, technical advances in hardware and software have made its implementation possible in a variety of clinical conditions . These benefits of computed tomography (CT) imaging have also introduced new challenges of increased radiation exposure to the patients . The CT manufacturers and users have focused mainly on a tube current time product (mAs)-based approach to lower dose because of a predictable linearity between radiation dose and tube current and its straightforward application in practice. However, the lower image quality on the traditional filtered back projection (FBP) reconstructed scans performed using a substantially reduced dose remains a major limitation of dose-modified scans . Major CT manufacturers have introduced iterative reconstruction techniques (IRTs) to reduce noise and artifact to improve image quality .
Hybrid IRT (h-IRT, iDose 4 ) functions in the projection domain and in image space for suppressing image noise and artifacts and improving geometry through a complex mathematical algorithm. The noisiest signals in the areas of low photon counts are identified first in the projection domain and suppressed by the iterative reconstruction process; remaining noise is then propagated in the image domain, where it is easy to locate and remove . To our knowledge, this reconstruction technique has been studied on CT scans of the abdomen acquired with a low tube voltage (80-kV) approach in smaller sized adult patients and shown the promising results of decreasing both radiation dose and contrast media while preserving image quality . Tube voltage (kV) has a quadratic relationship with the dose; its modification therefore achieves greater dose savings than mAs having more linearity with the dose. Low kV is often applied in high-contrast examinations such as CT angiographies, CT urography, arterial phase acquisitions, or kidney stone evaluation, where higher image noise can be accepted. However, low kV is not routinely practiced in low-contrast studies such as portal venous phase scans because of image quality concerns and inadequate familiarity with optimal kV selection and corresponding tube current modifications to preserve the diagnostic quality in patients of medium to larger body size . Therefore, the purpose of our study was to investigate the performance of h-IRT on image quality in dose-modified CT protocols using a low mAs approach in a phantom and in patients in comparison to FBP.
Materials and methods
Get Radiology Tree app to read full this article<
Rationale for Choosing the Level of IRT
Phantom study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
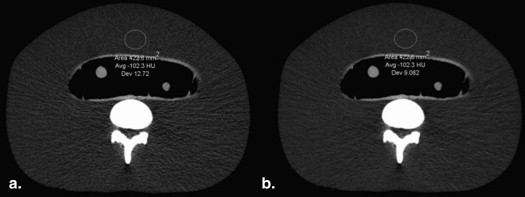
Noise Measurements Obtained in the Lower Torso Phantom at 100 and 120 kVp Using Different Tube Current-time Product Settings for FBP and h-IRT Images
100 kVp 120 kVp Technique 25 mAs 50 mAs 75 mAs 100 mAs 25 mAs 50 mAs 75 mAs 100 mAs FBP 30.4 ± 8.88 19.5 ± 4.8 15.9 ± 3.4 14.3 ± 2.9 19.7 ± 4.2 14.9 ± 3.9 12.7 ± 2.8 11.3 ± 2.1 h-IRT 1 21.1 ± 3.40 16.0 ± 3.1 13.8 ± 2.4 12.2 ± 2.6 15.3 ± 1.9 12.8 ± 3.1 11.1 ± 2.1 10.1 ± 2.0 h-IRT 2 20.5 ± 3.69 15.3 ± 3.0 12.8 ± 2.2 11.7 ± 2.1 13.9 ± 1.6 12.0 ± 2.7 10.1 ± 1.8 9.67 ± 1.9 h-IRT 3 19.0 ± 3.36 14.1 ± 3.0 11.8 ± 2.1 10.9 ± 2.0 12.9 ± 1.5 11.1 ± 2.8 9.33 ± 1.6 9.21 ± 1.8 h-IRT 4 17.6 ± 3.28 12.2 ± 2.8 10.9 ± 1.9 10.0 ± 1.9 12.1 ± 1.8 10.3 ± 2.5 8.73 ± 1.6 8.70 ± 1.8 h-IRT 5 15.8 ± 3.21 11.6 ± 2.4 10.1 ± 1.8 9.09 ± 1.9 11.0 ± 1.4 9.38 ± 2.1 8.18 ± 1.5 7.66 ± 1.6 h-IRT 6 14.0 ± 2.54 10.7 ± 2.6 8.87 ± 1.6 8.06 ± 1.4 9.93 ± 1.1 8.64 ± 2.2 7.10 ± 1.5 6.95 ± 1.4
FBP, filtered back projection; h-IRT, hybrid iterative reconstruction technique.
Scores are means ± standard deviations.
Get Radiology Tree app to read full this article<
Patient study
Get Radiology Tree app to read full this article<
CT technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image reconstruction
Get Radiology Tree app to read full this article<
Image Analysis
Quantitative evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Qualitative analysis
Get Radiology Tree app to read full this article<
Radiation dose measurements
Get Radiology Tree app to read full this article<
Statistical analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Quantitative and Qualitative Image Analysis
Get Radiology Tree app to read full this article<
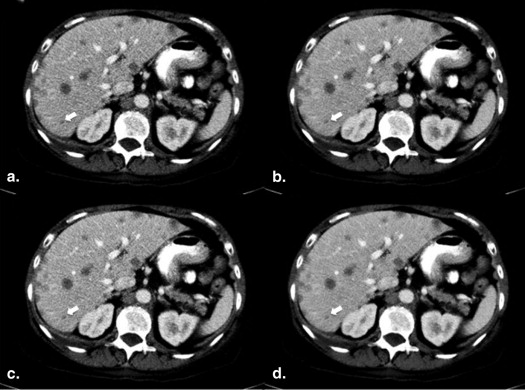
Table 2
Averaged Scores for Subjective Image Quality for Both Readers (R 1 /R 2)
Reconstruction Technique Minor Noise (Score <3) Minor Artifact (Score <3) Acceptable Overall
Image Quality (Score >3) FBP R 1 , 1.78 R 1 , 1.25 R 1 , 3.00 R 2 , 1.75 R 2 , 1.23 R 2 , 3.2 h-IRT level 1 R 1 , 1.46 R 1 , 1.19 R 1 , 3.12 R 2 , 1.55 R 2 , 1.23 R 2 , 3.32 h-IRT level 4 R 1 , 1.15 R 1 , 1.02 R 1 , 3.50 R 2 , 1.09 R 2 , 1.23 R 2 , 3.9 h-IRT level 5 R 1 , 1.03 R 1 , 1.02 R 1 , 3.92 R 2 , 1.09 R 2 , 1.19 R 2 , 3.96 FBP R 1 , 1.87 R 1 , 1.28 R 1 , 2.91 R 2 , 1.75 R 2 , 1.13 R 2 , 3.15 h-IRT level 4 R 1 , 1.13 R 1 , 1.03 R 1 , 3.62 R 2 , 1.17 R 2 , 1.08 R 2 , 3.74
FBP, filtered back projection; h-IRT, hybrid iterative reconstruction technique.
Images were considered diagnostic quality if subjective score for noise/artifacts <3, and overall IQ was >3.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 3, Axial dose-modified computed tomography obtained at 120 kVp and 120 mAs, size-specific dose estimate 9.12 mGy (window width, 451 Hounsfield units [HU]; window level, 102 HU) in a 36-year-old woman with mesenteric fibrosis ( white arrow ). Image quality on filtered back projection (a) was rated suboptimal because of increased noise. After applying hybrid reconstruction level 4 (b) , overall image quality was considered acceptable for diagnostic interpretation.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/Dosemodified256MDCToftheAbdomenUsingLowTubeCurrentandHybridIterativeReconstruction/2_1s20S1076633213003504.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Doses
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Dose Reduction on Dose-modified Abdominal CECT Scans Using Different Reconstruction Techniques
Author Dose Reduction Technique Mean Previous Dose CTDI (mGy) Mean Previous DLP (mGy-cm) Mean Dose Modified CTDI (mGy) Mean Dose Modified DLP (mGy-cm) Mean Body Mass Index/Body Weight (lb) Iterative Reconstruction Technique Sagara Noise index selection 25.0 1,193 17.0 860 26.8/— ASIR Hara noise index selection 22.0 894 12.0 470 24/— ASIR Kaza Low kVp (80) 20.79 1054 6.15 306 21.3/127 ASIR Kambadakone Noise index selection 12 577 7.7 380 —/135.08 ASIR Lee Low mAs (100) 7.0 365.7 3.5 182.8 19.1/121.2 IRIS Authors study Low mAs (100–120) 11.43 526 5.11 263 —/162.5 iDose
ASIR, adaptive statistical iterative reconstruction; CTDI, volume computed tomography dose index; DLP, dose-length product; IRIS, image reconstruction in space.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Boone J.M.: Multidetector CT opportunities, challenges, and concerns associated with scanners with 64 or more detector rows. Radiology 2006; 241: pp. 334-337.
2. Brenner D.J., Hall E.J.: Computed tomography: an increasing source of radiation exposure. N Engl J Med 2007; 357: pp. 2277-2284.
3. Berrington de González A., Mahesh M., Kim K., et. al.: Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med 2009; 169: pp. 2071-2077.
4. Thrall J.H.: Radiation exposure in CT scanning and risk: where are we?. Radiology 2012; 264: pp. 325-328.
5. Lee S.J., Park S.H., Kim A.Y., et. al.: A prospective comparison of standard-dose CT enterography and 50% reduced-dose CT enterography with and without noise reduction for evaluating Crohn disease. AJR Am J Roentgenol 2011; 197: pp. 50-57.
6. Fleischmann D., Boas F.E.: Computed tomography—old ideas and new technology. Eur Radiol 2011; 21: pp. 510-517.
7. Schindera S.T., Diedrichsen L., Müller H.C., et. al.: Iterative reconstruction algorithm for abdominal multidetector CT at different tube voltages: assessment of diagnostic accuracy, image quality, and radiation dose in a phantom study. Radiology 2011; 260: pp. 454-462.
8. Marin D., Nelson R.C., Schindera S.T., et. al.: Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm—initial clinical experience. Radiology 2010; 254: pp. 145-153.
9. Prakash P., Kalra M.K., Kambadakone A.K., et. al.: Reducing abdominal CT radiation dose with adaptive statistical iterative reconstruction technique. Invest Radiol 2010; 45: pp. 202-210.
10. Pickhardt P.J., Lubner M.H., Kim D.H., et. al.: Abdominal CT with model-based iterative reconstruction (MBIR): initial results of a prospective trial comparing ultralow-dose with standard-dose imaging. AJR Am J Roentgenol 2012; 199: pp. 1-9.
11. Kalra M.K., Woisetschläger M., Dahlström N., et. al.: Radiation dose reduction with sinogram affirmed iterative reconstruction technique for abdominal computed tomography. J Comput Assist Tomogr 2012; 36: pp. 339-346.
12. Nakaura T., Awaki K., Maruyama N., et. al.: Abdominal dynamic CT in patients with renal dysfunction: contrast agent dose reduction with low tube voltage and high tube current-time product settings at 256-detector row CT. Radiology 2011; 261: pp. 467-476.
13. Nakaura T., Nakamura S., Maruyama N., et. al.: Low contrast agent and radiation dose protocol for hepatic dynamic CT of thin adults at 256-detector row CT: effect of low tube voltage and hybrid iterative reconstruction algorithm on image quality. Radiology 2012; 264: pp. 445-454.
14. Guimarães L.S., Fletcher J.G., Harmsen W.S., et. al.: Appropriate patient selection at abdominal dual-energy CT using 80 kV: relationship between patient size, image noise, and image quality. Radiology 2010; 257: pp. 732-742.
15. Zalis M.E., Perumpillichira J.J., Kim J.Y., et. al.: Polyp Size at CT colonography after electronic subtraction cleansing in an anthropomorphic colon phantom. Radiology 2005; 236: pp. 118-124.
16. 2000.European Commission & The Office For Official Publications of the European CommunitiesLuxembourg www.drs.dk/guidelines/ct/quality/Download.htm Accessed July 10, 2013
17. Singh S., Kalra M.K., Hsieh J., et. al.: Abdominal CT: comparison of adaptive statistical iterative and filtered back projection reconstruction techniques. Radiology 2010; 257: pp. 373-383.
18. 2011.American Association of Physicists in MedicineCollege Park, MD
19. Tack D., Bohy P., Perlot I., et. al.: Suspected acute colon diverticulitis: imaging with low-dose unenhanced multi-detector row CT. Radiology 2005; 237: pp. 189-196.
20. Lee S.H., Kim M.J., Yoon C.S., et. al.: Radiation dose reduction with the adaptive statistical iterative reconstruction (ASIR) technique for chest CT in children: an intra-individual comparison. Eur J Radiol 2012; 81: pp. e938-e943. http://www.sciencedirect.com/science/article/pii/S0720048X1200280X
21. Liu W., Esler S.J., Kenny B.J., et. al.: Low-dose non enhanced helical CT of renal colic: assessment of ureteric stone detection and measurement of effective dose equivalent. Radiology 2000; 215: pp. 51-54.
22. Marin D., Nelson R.C., Barnhart H., et. al.: Detection of pancreatic tumors, image quality, and radiation dose during the pancreatic parenchymal phase: effect of a low-tube-voltage, high-tube-current CT technique—preliminary results. Radiology 2010; 256: pp. 450-459.
23. Kulkarni N.M., Uppot R.N., Eisner B.H., et. al.: Radiation dose reduction at multidetector CT with adaptive statistical iterative reconstruction for evaluation of urolithiasis: how low can we go?. Radiology 2012; 265: pp. 158-166.
24. Baker M.E., Dong F., Primak A., et. al.: Contrast-to-noise ratio and low-contrast object resolution on full- and low-dose MDCT: SAFIRE versus filtered back projection in a low-contrast object phantom and in the liver. AJR Am J Roentgenol 2012; 199: pp. 8-18.
25. Negi N., Yoshikawa T., Ohno Y., et. al.: Hepatic CT perfusion measurements: A feasibility study for radiation dose reduction using new image reconstruction method. Eur J Radiol 2012; 81: pp. 3048-3054.
26. Noël P.B., Fingerle A.A., Renger B., et. al.: Initial performance characterization of a clinical noise-suppressing reconstruction algorithm for MDCT. AJR Am J Roentgenol 2011; 197: pp. 1404-1409.
27. Hara A.K., Paden R.G., Silva A.C., et. al.: Iterative reconstruction technique for reducing body radiation dose at CT: feasibility study. AJR Am J Roentgenol 2009; 193: pp. 764-771.
28. Kaza R.K., Platt J.F., Al-Hawary M.H., et. al.: CT enterography at 80 kVp with adaptive statistical iterative reconstruction versus at 120 kVp with standard reconstruction: image quality, diagnostic adequacy and dose reduction. AJR Am J Roentgenol 2012; 198: pp. 1084-1092.
29. Sagara Y., Hara A., Pavlicek W., et. al.: Abdominal CT: comparison of low dose CT with adaptive statistical iterative reconstruction and routine dose CT with filtered back projection in 53 patients. AJR Am J Roentgenol 2010; 195: pp. 713-719.
30. Kambadakone A.R., Chaudhary N.A., Desai G.S., et. al.: Low dose MDCT and CT enterography of patients with Crohn disease: feasibility of adaptive statistical iterative reconstruction. AJR Am J Roentgenol 2011; 196: pp. W743-W752.
31. Yu L., Li H., Fletcher J.G., et. al.: Automatic selection of tube potential for radiation dose reduction in CT: a general strategy. Med Phys 2010; 37: pp. 234-243.
32. Iezzi R., Cotroneo A.R., Giammarino A., et. al.: Low-dose multidetector-row CT-angiography of abdominal aortic aneurysm after endovascular repair. Eur J Radiol 2011; 79: pp. 21-28.
33. Sahani D.V., Kalva S.P., Hahn P.F., et. al.: 16-MDCT angiography in living kidney donors at various tube potentials: impact on image quality and radiation dose. AJR Am J Roentgenol 2007; 188: pp. 115-120.
34. Namimoto T., Oda S., Utsunomiya D., et. al.: Improvement of image quality at low-radiation dose and low-contrast material dose abdominal CT in patients with cirrhosis: intraindividual comparison of low tube voltage with iterative reconstruction algorithm and standard tube voltage. J Comput Assist Tomogr 2012; 36: pp. 495-501.
35. Kalva S.P., Sahani D.V., Hahn P.F., et. al.: Using the K-edge to improve contrast conspicuity and to lower radiation dose with a 16-MDCT: a phantom and human study. J Comput Assist Tomogr 2006; 30: pp. 391-397.
36. Pinho D.F., Kulkarni N.M., Krishnaraj A., et. al.: Initial experience with single-source dual-energy CT abdominal angiography and comparison with single-energy CT angiography: image quality, enhancement, diagnosis and radiation dose. Eur J Radiol 2013; 23: pp. 351-359.