
Rationale and Objectives
This investigation aimed to evaluate the impact on treatment regimen and clinical outcome of dual-energy computed tomography (DECT) in patients with suspected gouty arthritis.
Materials and Methods
We retrospectively analyzed electronic medical records (EMR) of 39 patients (36 male, 3 female; age range, 36–85 years) who underwent DECT of peripheral joints because of suspected gouty arthritis. We assessed the prior medical history, lab results, treatment regimen, and medications before and after DECT, and changes in subjective severity of symptoms as stated by patients in the EMR. The presence of monosodium urate (MSU) crystals in the index joint was verified with DECT.
Results
Several patients had a prior diagnosis of gout ( n = 9), hyperuricemia ( n = 6), rheumatoid arthritis ( n = 3), or psoriatic arthritis ( n = 3). Elevated uric acid blood levels were detected in 32 patients (82%) before DECT. On DECT, MSU crystals were detected in 23 patients (59%). Of the 36 cases, the current treatment regimen was modified after DECT to gout-specific therapy in 22 cases and other rheumatic diseases were targeted in 14 cases. Several medications were prescribed more frequently based after DECT compared to before DECT imaging, including steroids ( n = 20 vs. n = 12, respectively), colchicine ( n = 13 vs. n = 4, respectively), and urate-lowering medication ( n = 18 vs. n = 11, respectively). A subjective reduction of clinical symptoms during cumulative follow-up was reported by 34 patients (87.2%).
Conclusions
Both positive and negative findings of MSU crystals on DECT have a significant impact on the treatment regimen and clinical outcome of patients with suspected gouty arthritis and facilitate differentiation from other rheumatic diseases.
Introduction
Gout is a medical condition characterized by severe pain attacks in joints usually caused by crystal arthropathy because of metabolic disorders. It is one of the most common arthropathies and is presently estimated to affect 1–2% of the adult population . A gout-specific therapy differs significantly from therapeutic regimens of other rheumatic or degenerative joint diseases . Therefore, an early and accurate diagnosis of gout is crucial for targeted treatment and rapid alleviation of symptoms.
The official guidelines of the European League Against Rheumatism state that synovial fluid aspiration is the present gold standard to establish the diagnosis . Nevertheless, this technique is invasive and may be difficult to perform in small joints, although it is considered the only method to definitely confirm the presence of monosodium urate (MSU) crystals and verify gout .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Design
Get Radiology Tree app to read full this article<
Medical Records
Get Radiology Tree app to read full this article<
DECT Imaging Protocol and Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Study Population and DECT Results
Get Radiology Tree app to read full this article<
TABLE 1
Patient Characteristics and Medical History
Parameter Patients Known gout 9 (23.1%) Known hyperuricemia 6 (15.4%) Known rheumatoid arthritis 3 (7.7%) Known psoriatic arthropathy 3 (7.7%) Known spondyloarthritis 1 (2.6%) Elevated uric acid 33 (84.6%)
Get Radiology Tree app to read full this article<
Patients’ Medical History and Findings on DECT
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
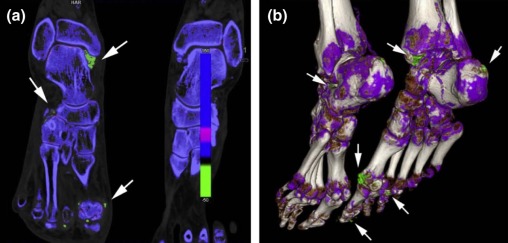
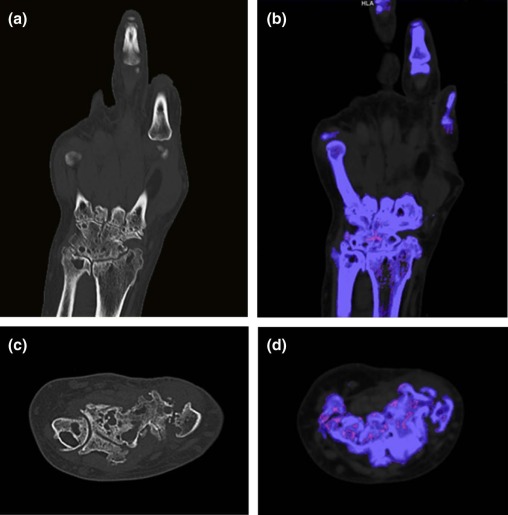
Imaging and Clinical Presentation of Index Joints
Get Radiology Tree app to read full this article<
Therapy Regimens
Get Radiology Tree app to read full this article<
TABLE 2
Treatment Regimens
Treatment Before DECT (Patients) MSU Crystal Positive (Patients) MSU Crystal Negative (Patients) After DECT (Patients) MSU Crystal Positive (Patients) MSU Crystal Negative (Patients) Corticosteroids 12 (30.8%) 7 5 20 (51.3%) 12 8 Colchicine 4 (10.3%) 3 1 13 (33.3%) 11 2 Urate-lowering medication 11 (28.2%) 8 3 18 (46.2%) 14 4 NSAIDs 16 (41.0%) 10 6 16 (41.0%) 12 4 Metamizole 4 (10.3%) 2 2 11 (28.2%) 5 6 Methotrexate 3 (7.7%) 1 2 3 (7.7%) 0 3 Biological agent 4 (10.3%) 2 2 4 (10.3%) 1 3 Opioid analgesic 2 (8.7%) 1 1 4 (10.3%) 3 1 Antibiotic therapy 1 (2.6%) 1 0 1 (2.6%) 0 1 Nonmedical treatment 0 0 0 4 (10.3%) 2 2
DECT, dual-energy computed tomography; MSU, monosodium urate; NSAIDs, nonsteroidal anti-inflammatory drugs.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Therapy Modification after DECT
Parameter All (Patients) MSU Crystals Positive (Patients) MSU Crystals Negative (Patients) Change in therapy after DECT 36 (92.3%) 21 (58.3%) 15 (41.7%) Change from other to gout-specific therapy 14 (35.9%) 11 (78.6%) 3 (21.4%) Maintained gout-specific therapy 8 (20.51%) 6 (75.0%) 2 (25.0%) Change from gout-specific to other therapy 2 (5.1%) 1 (50.0%) 1 (50.0%) Modified other therapy 12 (30.8%) 3 (25.0%) 9 (75.0%)
DECT, dual-energy computed tomography; MSU, monosodium urate.
Get Radiology Tree app to read full this article<
Outcome
Get Radiology Tree app to read full this article<
TABLE 4
Outcome/Follow-up
Follow-up Date Follow-up Data Available (Patients) Stated Improved Health Condition (Patients) Stated Stable or Worse Health Condition (Patients) At any follow-up date 39 (100%) 34 (87.2%) 5 (12.8%) At day of discharge 21 (53.8%) 19 (90.5%) 2 (9.5%) At <3 months follow-up 10 (25.6%) 8 (80%) 2 (20%) At >3 months follow-up 18 (46.2%) 11 (61.1%) 7 (38.9%)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kim K.Y., Ralph Schumacher H., Hunsche E., et. al.: A literature review of the epidemiology and treatment of acute gout. Clin Ther 2003; 25: pp. 1593-1617.
2. Smith E., Hoy D., Cross M., et. al.: The global burden of gout: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014; 73: pp. 1470-1476.
3. Zhu Y., Pandya B.J., Choi H.K.: Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum 2011; 63: pp. 3136-3141.
4. Perez-Ruiz F.: Treating to target: a strategy to cure gout. Rheumatology 2009; 48: pp. ii9-ii14.
5. Zhang W., Doherty M., Pascual E., et. al.: EULAR evidence based recommendations for gout. Part I: diagnosis. Report of a task force of the standing committee for international clinical studies including therapeutics (ESCISIT). Ann Rheum Dis 2006; 65: pp. 1301-1311.
6. Gordon C., Swan A., Dieppe P.: Detection of crystals in synovial fluids by light microscopy: sensitivity and reliability. Ann Rheum Dis 1989; 48: pp. 737-742.
7. Segal J.B., Albert D.: Diagnosis of crystal-induced arthritis by synovial fluid examination for crystals: lessons from an imperfect test. Arthritis Care Res 1999; 12: pp. 376-380.
8. Bongartz T., Glazebrook K.N., Kavros S.J., et. al.: Dual-energy CT for the diagnosis of gout: an accuracy and diagnostic yield study. Ann Rheum Dis 2015; 74: pp. 1072-1077. Epub ahead of print
9. Choi H.K., Burns L.C., Shojania K., et. al.: Dual energy CT in gout: a prospective validation study. Ann Rheum Dis 2012; 71: pp. 1466-1471.
10. Singh J.A.: Quality of life and quality of care for patients with gout. Curr Rheumatol Rep 2009; 11: pp. 154-160.
11. Khanna D., Fitzgerald J.D., Khanna P.P., et. al.: 2012 American College of Rheumatology guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res 2012; 64: pp. 1431-1446.
12. Neogi T., Hunter D.J., Chaisson C.E., et. al.: Frequency and predictors of inappropriate management of recurrent gout attacks in a longitudinal study. J Rheumatol 2006; 33: pp. 104-109.
13. Mikuls T.R., Curtis J.R., Allison J.J., et. al.: Medication errors with the use of allopurinol and colchicine: a retrospective study of a national, anonymous Internet-accessible error reporting system. J Rheumatol 2006; 33: pp. 562-566.
14. Doherty M., Jansen T.L., Nuki G., et. al.: Gout: why is this curable disease so seldom cured?. Ann Rheum Dis 2012; 71: pp. 1765-1770.
15. Perez-Ruiz F., Dalbeth N., Urresola A., et. al.: Gout. Imaging of gout: findings and utility. Arthritis Res Ther 2009; 11: pp. 232.
16. Gerster J.C., Landry M., Dufresne L., et. al.: Imaging of tophaceous gout: computed tomography provides specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 2002; 61: pp. 52-54.
17. Nicolaou S., Yong-Hing C.J., Galea-Soler S., et. al.: Dual-energy CT as a potential new diagnostic tool in the management of gout in the acute setting. AJR Am J Roentgenol 2010; 194: pp. 1072-1078.
18. Dalbeth N., Choi H.K.: Dual-energy computed tomography for gout diagnosis and management. Curr Rheumatol Rep 2013; 15: pp. 301.
19. Malik A., Schumacher H.R., Dinnella J.E., et. al.: Clinical diagnostic criteria for gout: comparison with the gold standard of synovial fluid crystal analysis. J Clin Rheumatol 2009; 15: pp. 22-24.
20. Schlesinger N.: Diagnosis of gout. Minerva Med 2007; 98: pp. 759-767.
21. Leiszler M., Poddar S., Fletcher A.: Clinical inquiry. Are serum uric acid levels always elevated in acute gout?. J Fam Pract 2011; 60: pp. 618-620.
22. Carter J.D., Kedar R.P., Anderson S.R., et. al.: An analysis of MRI and ultrasound imaging in patients with gout who have normal plain radiographs. Rheumatology 2009; 48: pp. 1442-1446.
23. Fitzgerald L., Donnellan J., Buckley O., et. al.: Duel energy CT imaging of tophaceous gout. Ir Med J 2013; 106: pp. 229.
24. Thiele R.G., Schlesinger N.: Diagnosis of gout by ultrasound. Rheumatology 2007; 46: pp. 1116-1121.