
Rationale and Objectives
Dual-source computed tomography enables bone removal on computed tomographic angiographic data on the basis of simultaneous dual-energy (DE) acquisition. The aim of this study was to evaluate the impact of this technique for the assessment of transcranial arteries. Therefore, the degree of stenosis of the transcranial arteries on DE computed tomographic angiography (CTA) with bone removal was compared to those on standard CTA and time-of-flight (TOF) magnetic resonance angiography (MRA).
Materials and Methods
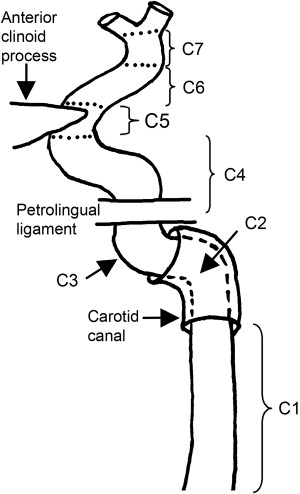
DE-CTA was performed using a dual-source computed tomographic scanner in 50 patients with suspected cerebrovascular disease. From the source images on DE-CTA, data sets with and without bone removal were reconstructed. TOF-MRA was performed on a 1.5-T scanner. Two blinded radiologists evaluated the segments of the internal carotid artery (C2–C7), the vertebral artery (V4), and the basilar artery for degree of stenosis. A five-step scale (0%–49%, 50%–69%, 70%–89%, 90%–99%, and 100% [occlusion]) for degree of stenosis was applied. Wilcoxon’s signed-rank test was used for statistical analysis.
Results
The degrees of stenosis on standard CTA were consistent with those on TOF-MRA in all segments. In contrast, DE-CTA showed significantly higher degrees of stenosis compared to standard CTA and TOF-MRA in both C2 segments ( P < .001). In addition, DE-CTA revealed a significantly higher degree of stenosis compared to standard CTA and TOF-MRA in the left C4 segment ( P < .01 and P < .005, respectively). All other segments showed no significant differences of stenosis among TOF-MRA, DE-CTA, and standard CTA.
Conclusions
Compared to TOF-MRA, standard CTA showed similar results. In contrast, DE-CTA revealed significant overestimation of stenosis for segments with close relations to bony structures as well as in calcified stenosis. Consequently, such findings on DE-CTA require confirmation with standard CTA or MRA to eliminate false-positive results.
Computed tomographic (CT) angiography (CTA) is a frequently used method for the evaluation of vessel pathologies of the supra-aortic and intracranial arteries. In particular for emergency assessment such as in acute stroke, computed tomography ( ) is used because of its wider availability, easier patient surveillance in the emergency setting, and fewer contraindications compared to magnetic resonance imaging (eg, metal implants, pacemakers) . Data from the literature emphasize the potential of noninvasive CTA for the assessment of acute and chronic cerebrovascular disease. The advantages of magnetic resonance angiography (MRA; eg, lack of radiation exposure) have already been described elsewhere , and this method is increasingly used in the evaluation of neurologic emergencies . Magnetic resonance imaging of the transcranial arteries is typically performed with time-of-flight (TOF) MRA .
In contrast to MRA, the delineation of vessels adjacent to bony structures (eg, the skull base) can be limited on CTA. Several techniques have been presented to eliminate bony structures from CT angiographic data sets on the basis of region-growth algorithms, section-by-section digital subtraction, and matched mask bone elimination . These bone-removal techniques have been assessed in several studies, which have shown partially correlative results . Therefore, none of these techniques has become standard in CTA of the transcranial arteries. The recent innovation of dual-source CT technology offers a new technical approach for bone removal in CTA . The two tubes of a dual-source scanner can be operated at different settings. This allows the simultaneous acquisition of two data sets at different tube voltages . Theoretically, bone and contrast-enhanced vessels can be identified by the different spectra of radiation absorption at two distinct tube voltages (eg, 80 and 140 kVp). Thereby, the selective elimination of bony structures and the preservation of contrast-enhanced vessels can be achieved .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Characteristics
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics ( n = 50)
Characteristic Value Age (y) 63.4 ± 15.3 Gender Male 27 (54%) Female 23 (46%) Symptoms Aphasia/dysarthria 14 (28%) Hemiplegia 15 (30%) Hemihypesthesia 6 (12%) Vision Impairment 3 (6%) Diplopia 6 (12%) Vertigo 9 (18%) Coma 2 (4%) Cardiovascular risk factors Arterial hypertension 33 (66%) Diabetes mellitus 11 (22%) Hyperlipidemia 19 (38%) Smoking 11 (22%) None 9 (18%)
Data are expressed as mean ± standard deviation or as number (percentage).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Examination Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison of Stenosis Grading
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Synopsis of Stenosis Scores ∗
Arterial Segment Standard CTA Bone-Removal DE-CTA TOF-MRA Right Left Right Left Right Left C2 1 44 42 40 40 44 45 2 0 2 4 4 0 0 3 0 0 0 0 0 0 4 0 0 0 0 0 0 5 2 2 2 2 2 1 C3 1 45 44 44 43 45 44 2 0 0 0 1 0 0 3 0 0 1 0 0 0 4 0 0 0 0 0 0 5 1 2 1 2 1 2 C4 1 45 41 45 38 45 44 2 0 2 0 3 0 0 3 0 1 0 1 0 0 4 0 0 0 1 0 0 5 1 2 1 3 1 2 C5 1 45 43 44 42 45 44 2 0 1 1 2 0 0 3 0 0 0 0 0 0 4 0 0 0 0 0 0 5 1 2 1 2 1 2 C6 1 45 44 44 43 45 44 2 0 0 0 0 0 0 3 0 0 0 0 0 0 4 0 0 0 0 0 0 5 1 2 2 3 1 2 C7 1 45 44 45 44 45 44 2 0 0 0 0 0 0 3 0 0 0 0 0 0 4 0 0 0 0 0 0 5 1 2 1 2 1 2 V4 1 46 46 45 45 46 45 2 0 0 0 1 0 1 3 0 0 1 0 0 0 Basilar artery 46 46 46
DE-CTA, dual-energy computed tomographic angiography; S-CTA, standard computed tomographic angiography; TOF-MRA, time-of-flight magnetic resonance angiography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 2, Mean stenosis score. Box plot of stenosis scoring of vessel segments with significant differences in stenosis grading between the three modalities (standard computed tomographic angiography [S-CTA], dual-energy computed tomographic angiography [DE-CTA], and time-of-flight magnetic resonance angiography [TOF-MRA]) according to North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria for stenosis grading (1 = 0%–49%, 2 = 50%–69%, 3 = 70%–89%, 4 = 90%–99%, and 5 = 100% [occlusion]). The box plot shows the significantly higher stenosis scores for the right (a) and left (b) C2 segment ( P < .001) and for the left C4 segment (c) on DE-CTA compared to S-CTA ( P < .01) and TOF-MRA ( P < .005).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/DualEnergyCTAwithBoneRemovalforTranscranialArteries/1_1s20S1076633209003043.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Kloska S.P., Dittrich R., Fischer T., et. al.: Perfusion CT in acute stroke: prediction of vessel recanalization and clinical outcome in intravenous thrombolytic therapy. Eur Radiol 2007; 17: pp. 2491-2498.
2. Adams H.P., del Zoppo G., Alberts M.J., et. al.: Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups. Stroke 2007; 38: pp. 1655-1711.
3. Kloska S.P., Nabavi D.G., Gaus C., et. al.: Acute stroke assessment with CT: do we need multimodal evaluation?. Radiology 2004; 233: pp. 79-86.
4. Villablanca J.P., Nael K., Habibi R., Nael A., Laub G., Finn J.P.: 3 T contrast-enhanced magnetic resonance angiography for evaluation of the intracranial arteries: comparison with time-of-flight magnetic resonance angiography and multislice computed tomography angiography. Invest Radiol 2006; 41: pp. 799-805.
5. Bash S., Villablanca J.P., Jahan R., et. al.: Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography. AJNR Am J Neuroradiol 2005; 26: pp. 1012-1021.
6. Randoux B., Marro B., Koskas F., Chiras J., Dormont D., Marsault C.: Proximal great vessels of aortic arch: comparison of three-dimensional gadolinium-enhanced MR angiography and digital subtraction angiography. Radiology 2003; 229: pp. 697-702.
7. Remonda L., Senn P., Barth A., Arnold M., Löblad K.O.: Schroth. Contrast-enhanced 3D angiography of the carotid artery; comparison with conventional digital subtraction angiography. AJNR Am J Neuroradiol 2002; 23: pp. 213-219.
8. Kalowska E., Rostrup E., Rosenbaum S., Petersen P., Paulson O.B.: Acute MRI changes in progressive ischemic stroke. Eur Neurol 2008; 59: pp. 229-236.
9. Okahara M., Kiyosue H., Yamashita M., et. al.: Diagnostic accuracy of magnetic resonance angiography for cerebral aneurysms in correlation with 3D-digital subtraction angiographic images: a study of 133 aneurysms. Stroke 2002; 33: pp. 1803-1808.
10. Choi C.G., Lee D.H., Lee J.H., et. al.: Detection of intracranial atherosclerotic steno-occlusive disease with 3D time-of-flight magnetic resonance angiography with sensitivity encoding at 3T. AJNR Am J Neuroradiol 2007; 28: pp. 439-446.
11. Lell M.M., Ditt H., Panknin C., et. al.: Cervical CT angiography comparing routine noncontrast and a late venous scan as masks for automated bone subtraction: feasibility study and examination of the influence of patient motion on image quality. Invest Radiol 2008; 43: pp. 27-32.
12. Lell M.M., Ditt H., Panknin C., et. al.: Bone-subtraction CT angiography: evaluation of two different fully automated image-registration procedures for interscan motion compensation. AJNR Am J Neuroradiol 2007; 28: pp. 1362-1368.
13. Flohr T.G., McCollough C.H., Bruder H., et. al.: First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol 2006; 16: pp. 256-268.
14. Johnson T.R., Krauss B., Sedlmair M., et. al.: Material differentiation by dual energy CT: initial experience. Eur Radiol 2007; 17: pp. 1510-1517.
15. Osborn A.G.: Diagnostic cerebral angiography.2nd ed1999.Lippincott Williams & WilkinsPhiladelphia, PA 58
16. North American Symptomatic Carotid Endarterectomy Trial (NASCET) Investigators: Clinical alert. benefit of carotid endarterectomy for patients with high-grade stenosis of the internal carotid artery. Stroke 1991; 22: pp. 816-817.
17. Brittenden J., Murie J.A., Jenkins A.M., Ruckley C.V., Bradbury A.W.: Carotid endarterectomy before and after publication of randomized controlled trials. Br J Surg 1999; 86: pp. 206-210.
18. Hacklander T., Wegner H., Hoppe S., et. al.: Agreement of multislice CT angiography and MR angiography in assessing the degree of carotid artery stenosis in consideration of different methods of postprocessing. J Comput Assist Tomogr 2006; 30: pp. 433-442.
19. Easton J.D., Wilterdink J.L.: Carotid endarterectomy: trials and tribulations. Ann Neurol 1994; 35: pp. 5-17.
20. Romijn M., Gratama van Andel H.A., van Walderveen M.A., et. al.: Diagnostic accuracy of CT angiography with matched mask bone elimination for detection of intracranial aneurysms: comparison with digital subtraction angiography and 3D rotational angiography. AJNR Am J Neuroradiol 2008; 29: pp. 134-139.
21. van Straten M., Venema H.W., Streekstra G.J., Majoie C.B., den Heeten G.J., Grimbergen C.A.: Removal of bone in CT angiography of the cervical arteries by piecewise matched mask bone elimination. Med Phys 2004; 31: pp. 2924-2933.
22. Sarikaya B., Sarikaya S., Deniz F.E., Acu B., Kablan Y., Firat M.M.: Unregistered subtracted CT angiography for the visualization of intracranial arteries at or near the skull base: preliminary experience. Diagn Interv Radiol 2007; 13: pp. 105-108.
23. Tomandl B.F., Hammen T., Klotz E., Ditt H., Stemper B., Lell M.: Bone-subtraction CT angiography for the evaluation of intracranial aneurysms. AJNR Am J Neuroradiol 2006; 27: pp. 55-59.
24. Gratama van Andel H.A., Venema H.W., Streekstra G.J., et. al.: Removal of bone in CT angiography by multiscale matched mask bone elimination. Med Phys 2007; 34: pp. 3711-3723.
25. Loeckx D., Coudyzer W., Maes F., et. al.: Nonrigid registration for subtraction CT angiography applied to the carotids and cranial arteries. Acad Radiol 2007; 14: pp. 1562-1576.
26. Binaghi S., Maeder P., Uske A., Meuwly J.Y., Devuyst G., Meuli R.A.: Three-dimensional computed tomography angiography and magnetic resonance angiography of carotid bifurcation stenosis. Eur Neurol 2001; 46: pp. 25-34.
27. Lell M., Fellner C., Baum U., et. al.: Evaluation of carotid artery stenosis with multisection CT and MR imaging: influence of imaging modality and postprocessing. AJNR Am J Neuroradiol 2007; 28: pp. 104-110.
28. Tran D.N., Straka M., Roos J.E., Napel S., Fleischmann D.: Dual-energy CT discrimination of iodine and calcium: experimental results and implications for lower extremity CT angiography. Acad Radiol 2009; 16: pp. 160-171.
29. Watanabe Y., Uotani K., Nakazawa T., et. al.: Dual-energy direct bone removal CT angiography for evaluation of intracranial aneurysm or stenosis: comparison with conventional digital subtraction angiography. Eur Radiol 2008; 11: pp. 1213-1215.