
Rationale and Objectives
The dual-energy radiographic technique has been proved to be clinically useful in the thorax. Herein, we attempt to apply this technique to the abdomen and pelvis in the context of renal colic.
Materials and Methods
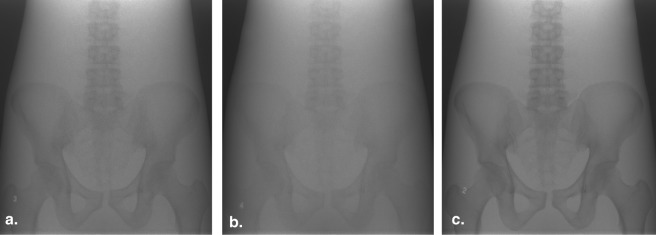
The visibility of renal calculi were assessed using various dual energy peak kilovoltage combination radiographs applied to standard phantoms.
Results
This technique demonstrates a higher than acceptable radiation dosage required to optimize the image quality and the optimized diagnostic quality is inferior to that of the standard Kidneys, Ureters, and Bladder radiograph.
Conclusions
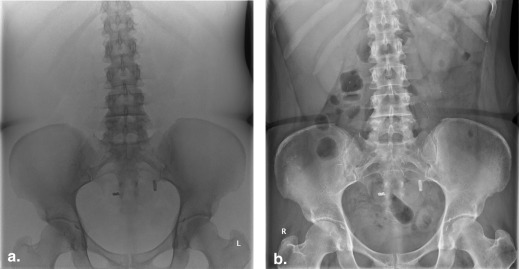
The dual-energy radiographic technique could not better identify the radiopaque renal calculi. Limiting technical considerations include the increased subcutaneous and peritoneal adipose tissue and the limited contrast between the soft tissue and underlying calculi.
Kidney stones affect up to 5%–10% of the general population and are a common emergency presentation in developed nations. They have been associated with improved standards of living, the male sex, and a peak incidence at around 30 years of age . At least 50% of patients will have recurrences. Kidney stones vary in composition and are broadly categorized as calcium-containing stones that are radiopaque and noncalcareous stones including struvite and cystine which have variable radiographic opacity and conspicuity; pure uric acid stones are lucent. Radiologic evaluation plays an important role in determining the appropriate management .
In acute presentations of possible renal calculus, a low-dose unenhanced computed tomography (CT) of the abdomen and pelvis, which includes the Kidneys, Ureters, and Bladder (KUB), is currently the gold standard to assess for stone size, location, and possible complications. Even after treatment, a subset of patients will have recurrent calculi that can lead to chronic renal disease and significant morbidity. At our institution, patients with suspected or known recurrent urinary stone disease undergo at least a plain radiograph and/or a low-dose unenhanced multidetector CT. The low-dose CT examination is not benign and can impart ∼3.2 mSv of radiation per scan versus 0.7 mSv from a plain radiographic KUB. Some patients will have undergone multiple CT examinations for recurrent stone disease. Considering that stones frequently first appear in patients of reproductive age, strategies to minimizing radiation exposure are desirable. A lower dose alternative is to obtain a plain radiograph KUB to assess for stones. However, this method is limited by the radio-opacity of the stone [only 59% of urinary stones are radiodense ], and often small stones are obscured by overlying soft tissue and bowel stool and gas , making this a low-sensitivity examination at 45%–59% .
Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results and discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Asplin J.R., Favus M.J., Coe F.L.: Nephrolithiasis.Brenner B.M.Brenner and Rector’s The kidney.1996.SaundersPhiladelphia:pp. 1893-1935.
2. Stamatelou K.K., Francis M.E., Jones C.A., et. al.: Time trends in reported prevalence of kidney stones in the United States: 1976–1994. Kidney International 2003; 63: pp. 1817-1823.
3. Yen P., Baerlocher M.: Five things to know about imaging in urolithiasis. Can Med Ass J 2011; 183: pp. 2133.
4. Levine J.A., Neitlich J., Verga M., et. al.: Ureteral calculi in patients with flank pain: correlation of plain radiography with unenhanced helical CT. Radiology 1997; 204: pp. 27-31.
5. Sommer F.G., Brody W.R., Gross D., et. al.: Renal imaging with dual energy projection radiography. American Journal of Roentgenology 1982; 138: pp. 317-322.
6. Sabol J.M., Wheeldon S.J., Jabri K.N.: Simulated and experimental technique optimization of dual-energy radiography: abdominal imaging applications.Flynn M.J.Hsieh J.Physics of medical imaging.2006.Proceedings of SPIE Medical Imagingpp. 6142. 61421J-1-12
7. Lehmann L.A., Alvarez R.A., Macovski A., et. al.: Generalized image combinations in dual kVp digital radiography. Medical Physics 1981; 8: pp. 659-667.