
Rationale and Objectives
Automatic bone and plaque subtraction (BPS) in computed tomographic angiographic (CTA) examinations using dual-energy CT (DECT) remains challenging because of beam-hardening artifacts in the shoulder region and close proximity of the internal carotid artery to the base of the skull. The selection of the tube voltage combination in dual-source CT influences the spectral separation and the susceptibility for artifacts. The purpose of this study was to assess which tube voltage combination leads to an optimal image quality of head and neck DECT angiograms after bone subtraction.
Materials and Methods
Fifty-one patients received tin-filter–enhanced DECT angiograms of the supra-aortic arteries using two voltage protocols: 24 patients were studied using 80/Sn140 kV and 27 using a 100/Sn140 kV protocol, both protocols with an additional tin filter. A commercially available DE-CTA BPS algorithm was used. Artificial vessel erosions in BPS maximum intensity projections (four-level Likert scale with CTA source data as reference) and vessel signal-to-noise ratio (SNR) were assessed in the level of the shoulders and the base of the skull in each patient and compared.
Results
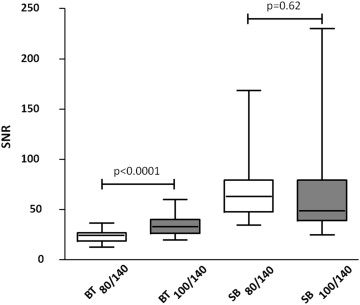
At the level of the shoulder, 100/Sn140 kV achieved higher SNR (23.4 ± 6.4 at 80/Sn140 kV vs. 35.1 ± 11.8 at 100/Sn140 kV; P < .0001) with less erosions (erosion score 3.9 ± 0.4 in 80/Sn140 kV vs. 2.1 ± 1.3 in 100/Sn140 kV; P < .0001) than 80/Sn140 kV. At the level of the skull base, erosion scores and objective image quality of arterial segments were comparable with both protocols ( P = .14).
Conclusions
The 100/Sn140 kV protocol achieved more favorable results for BPS of the supra-aortic arteries than the 80/Sn140 kV protocol.
Computed tomography angiography (CTA) and magnetic resonance imaging (MRI) are the two most important imaging modalities for noninvasive angiographic studies of the supra-aortic vessels . A major advantage of CT over MRI is the detection of calcified plaques which is clinically relevant for risk stratification in patients with asymptomatic hemodynamically relevant internal carotid artery stenosis and for planning interventions or surgery . However, visibility of arterial segments is limited in regions with close contact to bones and extensive calcifications when using conventional CTA images. Furthermore, it is impossible to create angiographic-like maximum intensity projection (MIP) images from plain CT data sets because of superposition of bones and calcified plaques. Automatic bone and plaque subtraction (BPS) by dual-energy CTA (DE-CTA) has become an established method to suppress bones and calcified plaques in the final CTA image and to provide MIP reconstructions of the supra-aortic arteries similar to angiograms created by MRA . However, this technique is still limited in challenging anatomic regions such as the shoulders and at the base of the skull or in the presence of heavily calcified plaques where artificial vessel erosions may occur .
Second-generation dual-source CT systems (Somatom Definition Flash; Siemens) feature a tin filter which allows further hardening of the high energy spectrum. Thus, a combination of 100/140 kV with tin filter (100/Sn140 kV) achieves a comparable spectral separation as 80/140 kV without tin filter while providing lower noise levels in the low-energy spectrum , which may improve image quality in the shoulder region. On the other hand, a combination of 80/140 kV with tin filter (80/Sn140 kV) leads to a further improved spectral separation, which might improve the accuracy of BPS in the base of the skull because of a larger difference of the calcium and iodine slope. Thus, both protocols appear attractive for DE-CTA of the supra-aortic vessels, and it remains uncertain which voltage combination is optimal.
Get Radiology Tree app to read full this article<
Material and methods
Patients
Get Radiology Tree app to read full this article<
CT Data Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Data Reconstruction
Get Radiology Tree app to read full this article<
Image Postprocessing
Get Radiology Tree app to read full this article<
Quantitative Image Analysis
Get Radiology Tree app to read full this article<
Qualitative Image Analysis
Get Radiology Tree app to read full this article<
Dose Measurements
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Qualitative Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
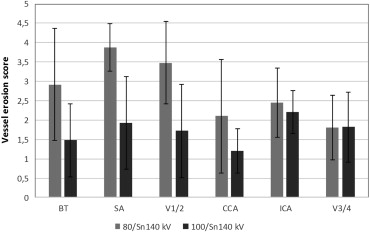
Table 1
Subjective Vessel Erosion Score (1–4) Per Vessel Segment
Location 80/Sn140 kV 100/Sn140 kV_P_ Value BT 2.92 ± 1.44 1.48 ± 0.94 <.05 SA 3.88 ± 0.61 1.93 ± 1.20 <.05 V1/2 3.48 ± 1.07 1.72 ± 1.20 <.05 CCA 2.10 ± 1.46 1.20 ± 0.57 <.05 ICA 2.45 ± 0.90 2.21 ± 0.55 .29 V3/4 1.81 ± 0.83 1.82 ± 0.91 .95
BT, brachiocephalic trunk; CCA, common carotid artery; ICA, internal carotid artery embedded in the bony canal of the scull base (C2–C6); SA, subclavian artery; V1/2 ostium, V1 and V2 segments of the vertebral artery; V3/4, V3 and V4 segments of the vertebral artery.
A lower score indicates good delineation of the vessel lumen. Data are presented as mean plus standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Table 2
Radiation Dose as Reported by the Computed Tomography Scanner (CTDI vol and DLP) and Estimated Effective Dose (ED)
Feature CTDI vol (mGy) DLP (mGy × cm) ED (mSv) 80/Sn140 kV 8.1 ± 0.5 312.4 ± 24.5 1.50 ± 0.12 100/Sn140 kV 9.2 ± 0.5 350.0 ± 28.6 1.68 ± 0.14
CTDI vol , volume CT dose index; DLP, dose–length product.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Chappell F.M., Wardlaw J.M., Young G.R., et. al.: Carotid artery stenosis: accuracy of noninvasive tests-individual patient data meta-analysis. Radiology 2009; 251: pp. 493-502.
2. Kwee R.M.: Systematic review on the association between calcification in carotid plaques and clinical ischemic symptoms. J Vasc Surg 2010; 51: pp. 1015-1025.
3. Morhard D., Fink C., Graser A., et. al.: Cervical and cranial computed tomographic angiography with automated bone removal: dual energy computed tomography versus standard computed tomography. Invest Radiol 2009; 44: pp. 293-297.
4. Deng K., Liu C., Ma R., et. al.: Clinical evaluation of dual-energy bone removal in CT angiography of the head and neck: comparison with conventional bone-subtraction CT angiography. Clin Radiol 2009; 64: pp. 534-541.
5. Thomas C., Korn A., Krauss B., et. al.: Automatic bone and plaque removal using dual energy CT for head and neck angiography: feasibility and initial performance evaluation. Eur J Radiol 2010; 76: pp. 61-67.
6. Zhang Z., Berg M.H., Ikonen A.E., et. al.: Carotid artery stenosis: reproducibility of automated 3D CT angiography analysis method. Eur Radiol 2004; 14: pp. 665-672.
7. Lell M., Anders K., Klotz E., et. al.: Clinical evaluation of bone-subtraction CT angiography (BSCTA) in head and neck imaging. Eur Radiol 2006; 16: pp. 889-897.
8. Lell M.M., Anders K., Uder M., et. al.: New techniques in CT angiography. Radiographics 2006; 26: pp. S45-S62. Review
9. Lell M.M., Kramer M., Klotz E., et. al.: Carotid computed tomography angiography with automated bone suppression: a comparative study between dual energy and bone subtraction techniques. Invest Radiol 2009; 44: pp. 322-328.
10. Schulz B., Kuehling K., Kromen W., et. al.: Automatic bone removal technique in whole-body dual-energy CT angiography: performance and image quality. Am J Roentgenol 2012; 199: pp. W646-W650.
11. Johnson T.R., Krauss B., Sedlmair M., et. al.: Material differentiation by dual energy CT: initial experience. Eur Radiol 2007; 17: pp. 1510-1517.
12. Graser A., Johnson T.R., Chandarana H., et. al.: Dual energy CT: preliminary observations and potential clinical applications in the abdomen. Eur Radiol 2008; 19: pp. 13-23.
13. Lell M.M., Hinkmann F., Nkenke E., et. al.: Dual energy CTA of the supraortic arteries: technical improvements with a novel dual source CT system. Eur J Radiol 2010; 76: pp. e6-e12.
14. Primak A.N., Ramirez Giraldo J.C., Liu X., et. al.: Improved dual-energy material discrimination for dual-source CT by means of additional spectral filtration. Med Phys 2009; 36: pp. 1359-1369.
15. Primak A.N., Giraldo J.C., Eusemann C.D., et. al.: Dual-source dual-energy CT with additional tin filtration: dose and image quality evaluation in phantoms and in vivo. Am J Roentgenol 2010; 195: pp. 1164-1174.
16. Thomas C., Krauss B., Ketelsen D., et. al.: Differentiation of urinary calculi with dual energy CT: effect of spectral shaping by high energy tin filtration. Invest Radiol 2010; 45: pp. 393-398.
17. Mnyusiwalla A, Aviv RI, Symons SP. Radiation dose from multidetector row CT imaging for acute stroke. Neuroradiology 51(10):635–640.
18. Tomandl B.F., Hammen T., Klotz E., et. al.: Bone-Subtraction CT angiography for the evaluation of intracranial aneurysms. Am J Neuroradiol 2006; 27: pp. 55-59.
19. Watanabe Y., Uotani K., Nakazawa T., et. al.: Dual-energy direct bone removal CT angiography for evaluation of intracranial aneurysm or stenosis: comparison with conventional digital subtraction angiography. Eur Radiol 2009; 19: pp. 1019-1024.
20. Uotani K., Watanabe Y., Higashi M., et. al.: Dual-energy CT head bone and hard plaque removal for quantification of calcified carotid stenosis: utility and comparison with digital subtraction angiography. Eur Radiol 2009; 19: pp. 2060-2065.
21. Thomas C., Korn A., Ketelsen D., et. al.: Automatic lumen segmentation in calcified plaques: dual-energy CT versus standard reconstructions in comparison with digital subtraction angiography. Am J Roentgenol 2010; 194: pp. 1590-1595.
22. Korn A., Bender B., Thomas C., et. al.: Dual energy CTA of the carotid bifurcation: advantage of plaque subtraction for assessment of grade of the stenosis and morphology. Eur J Radiol 2011; 80: pp. e120-e125.
23. Flohr T.G., McCollough C.H., Bruder H., et. al.: First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol 2006; 16: pp. 256-268.