
Rationale and Objectives
The aim of this study was to assess the feasibility of dynamic contrast-enhanced ultra–high-field breast imaging at 7 Tesla.
Material and Methods
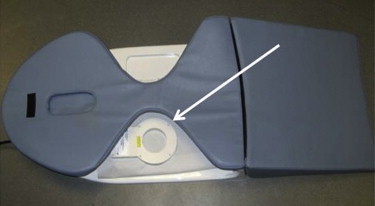
A total of 15 subjects, including 5 patients with histologically proven breast cancer, were examined on a 7 Tesla whole-body magnetic resonance imaging system using a unilateral linearly polarized single-loop coil. Subjects were placed in prone position on a biopsy support system, with the coil placed directly below the region of interest. The examination protocol included the following sequences: 1) T2-weighted turbo spin echo sequence; 2) six dynamic T1-weighted spoiled gradient-echo sequences; and 3) subtraction imaging.
Results
Contrast-enhanced T1-weighted imaging at 7 Tesla could be obtained at high spatial resolution with short acquisition times, providing good image accuracy and a conclusively good delineation of small anatomical and pathological structures. T2-weighted imaging could be obtained with high spatial resolution at adequate acquisition times. Because of coil limitations, four high-field magnetic resonance examinations showed decreased diagnostic value.
Conclusions
This first scientific approach of dynamic contrast-enhanced breast magnetic resonance imaging at 7 Tesla demonstrates the complexity of ultra–high-field breast magnetic resonance imaging and countenances the implementation of further advanced bilateral coil concepts to circumvent current limitations from the coil and ultra–high-field magnetic strength.
Since the early 1980s, contrast-enhanced magnetic resonance imaging (MRI) of the breast has gone through substantial developments. The first MRI exams were performed on 0.2 Tesla MRI scanners in supine position using a body coil . Through the years, there have been major improvements involving the introduction of dedicated breast coils as well as of specific examination protocols. With the increase of the magnetic field strength, the associated higher signal-to-noise ratio (SNR) has helped in the acquisition of high spatial resolution at high temporal resolution .
Currently, 1.5 Tesla breast MRI is considered the worldwide clinical standard. However, 3 Tesla breast imaging has been nearing clinical readiness within the last few years . Recent studies correlating 1.5 Tesla and 3 Tesla breast MRI demonstrate better image quality of the 3 Tesla breast images, yet also alluding to new obstacles associated with high magnetic field strength, such as inhomogeneities of the radiofrequency (RF) field and RF-related limitations of specific absorption rate (SAR) . There are theoretical advantages of using even higher field strengths than 3 Tesla, including higher SNR and higher spatial resolution images.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods and materials
Study Population
Get Radiology Tree app to read full this article<
Scanner and Coil Systems
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Examination at 7 Tesla
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
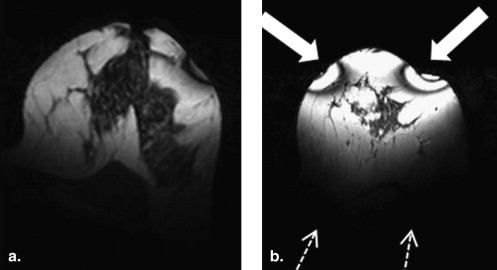
Dynamic T1-weighted imaging and subtraction imaging
Get Radiology Tree app to read full this article<
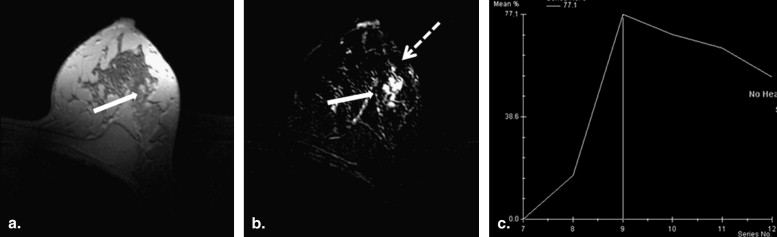
Get Radiology Tree app to read full this article<
T2-weighted Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. El Yousef S.J., Duchesneau R.H., Alfidi R.J., et. al.: Magnetic resonance imaging of the breast. Work in progress. Radiology 1984; 150: pp. 761-766.
2. Kuhl C.K.: Breast MR imaging at 3T. Magnet Res Imaging Clin N Am 2007; 15: pp. 315-320.
3. Pinker K., Grabner G., Bogner W., et. al.: A combined high temporal and high spatial resolution 3 Tesla MR imaging protocol for the assessment of breast lesions initial results. Invest Radiol 2009; 44: pp. 553-558.
4. Kuhl C.K., Jost P., Morakkabati N., et. al.: Contrast-enhanced MR imaging of the breast at 3.0 and 1.5 T in the same patients: initial experience. Radiology 2006; 239: pp. 666-676.
5. Kuhl C.K., Kooijman H., Gieseke J., et. al.: Effect of B1 inhomogeneity on breast MR imaging at 3.0 T. Radiology 2007; 244: pp. 929-930.
6. Kollia K., Maderwald S., Putzki N., et. al.: First clinical study on ultra-high-field MR imaging in patients with multiple sclerosis: comparison of 1.5T and 7T. AJNR Am J Neuroradiol 2009; 30: pp. 699-702.
7. Maderwald S., Ladd S., Gizewski E., et. al.: To TOF or not to TOF: strategies for non-contrast-enhanced intracranial MRA at 7 T. Magnet Res Materials Phys Biol Med 2008; 21: pp. 159-167.
8. Mönninghoff C., Maderwald S., Theysohn J.M., et. al.: Evaluation of intracranial aneurysms with 7 T versus 1.5 T time-of-flight MR angiography; initial experience. Beurteilung von intrakraniellen Hirnarterienaneurysmen mit 7 Tesla versus 1,5 Tesla-time-of-flight-MR-Angiografie. erste Erfahrungen 2009; 181: pp. 16-23.
9. Snyder C.J., DelaBarre L.J., Metzger P., et. al.: Initial results of cardiac imaging at 7 tesla. Magnet Res Med 2009; 61: pp. 517-524.
10. Vaughan J.T., Snyder C.J., DelaBarre L.J., et. al.: Whole-body imaging at 7T: preliminary results. Magn Reson Med 2009; 61: pp. 244-248.
11. Hecht E.M., Lee R.F., Taouli B., et. al.: Perspectives on body MR imaging at ultrahigh field. Magn Reson Imaging Clin N Am 2007; 15: pp. 449-465.
12. American College of Radiology: Breast Imaging Reporting and Data System Atlas (BI-RADS– MRI).2003.American College of RadiologyReston, VA
13. Dietrich O., Raya J.G., Reeder S.B., et. al.: Measurement of signal-to-noise ratios in MR images: influence of multichannel coils, parallel imaging, and reconstruction filters. J Magn Reson Imaging 2007; 26: pp. 375-385.
14. Kraff O., Theysohn J.M., Maderwald S., et. al.: High-Resolution MRI of the Human Parotid Gland and Duct at 7 Tesla. Investigative Radiol 2009; 44: pp. 518-524.
15. Merkle E.M., Dale B.M.: Abdominal MRI at 3.0 T: the basics revisited. Am J Roentgenol 2006; 186: pp. 1524-1532.
16. Azlan C.A., Di Giovanni P., Ahearn T.S., et. al.: B1 transmission-field inhomogeneity and enhancement ratio errors in dynamic contrast-enhanced MRI (DCE-MRI) of the breast at 3T. J Magn Reson Imaging 2010; 31: pp. 234-239.
17. Akisik F.M., Sandrasegaran K., Aisen A.M., et. al.: Abdominal MR imaging at 3.0 T. Radiographics 2007; 27: pp. 1433-1444.
18. Berg W.A., Gutierrez L., NessAiver M.S., et. al.: Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 2004; 233: pp. 830-849.
19. Bernstein M.A., Huston J., Ward H.A.: Imaging artifacts at 3.0T. J Magnet Res Imaging 2006; 24: pp. 735-746.
20. Hatakenaka M., Soeda H., Yabuuchi H., et. al.: Apparent diffusion coefficients of breast tumors: clinical application. Magnet Res Med Sci 2008; 7: pp. 23-29.
21. Sinha S., Sinha U.: Recent advances in breast MRI and MRS. NMR Biomed 2008; 22: pp. 3-16.
22. Mountford C.L.C., Malycha P., Russell P.: Proton spectroscopy provides accurate pathology on biopsy and in vivo. J Magnet Res Imaging 2006; 24: pp. 459-477.
23. Bolan P.J., Meisamy S., Baker E.H., et. al.: In vivo quantification of choline compounds in the breast with 1H MR spectroscopy. Magnet Res Med 2003; 50: pp. 1134-1143.
24. Bartella L., Huang W.: Proton (1H) MR spectroscopy of the breast. Radiographics 2007; 27: pp. S241-S252.
25. Meisamy S., Bolan P.J., Baker E.H., et. al.: Adding in vivo quantitative 1H MR spectroscopy to improve diagnostic accuracy of breast MR imaging: preliminary results of observer performance study at 4.0 T. Radiology 2005; 236: pp. 465-475.