
Rationale and Objectives
Dynamic flow ultrasound (DFUS) is a new color Doppler imaging method with better B-mode imaging and fewer blooming effects and color noises. This study was designed to compare the imaging quality of vessel signals in thoracic lesions using DFUS, color Doppler US (CDUS), and power Doppler US (PDUS).
Materials and Methods
Thirty-four patients with thoracic lesions abutting pulsatile organs [heart ( n = 13), aorta ( n = 14) and pulmonary artery ( n = 7)] and undergoing complete chest US examinations were included to assess the imaging quality about vessel signals, blooming effect, color noise, and the influence of decision in needle biopsy between different US modes.
Results
Our results showed that DFUS, CDUS, and PDUS could all demonstrate the vessel signals clearly (all P > .05). However, when focusing on the blooming effect and color noise, DFUS showed the more superior imaging quality than CDUS and PDUS (all P ≤ .001); and acceptable blooming effects/color noise were found with 100% (34/34)/97% (33/34), 35% (12/34)/68% (23/34), and 26% (9/34)/38% (13/34) in DFUS, CDUS, and PDUS, respectively. Especially, in the assessment of decision making for percutaneous needle biopsy, DFUS had the less influence than CDUS and PDUS (3% [1/33] versus 29% [10/34] and 3% [1/33] versus 38% [13/34], both P < .01).
Conclusions
We concluded that DFUS has a clearly more superior imaging quality than CDUS and PDUS in demonstrating the vessel signals of thoracic lesions, with less blooming effect and color noise.
Chest ultrasound (US) examination and US-guided needle biopsy have been widely used to assess and diagnose thoracic lesions abutting the chest wall with promising results, even in critically ill patients ( ). However, the use of conventional gray-scale US only is often limited in the assessment of vessel signals in thoracic lesions because US-guided needle biopsy for pulmonary lesions is somewhat risky, especially the biopsy of uncommon and unknown mediastinal tumors and pulmonary consolidations ( ). Thus the real-time visualization of vessel signals during the performance of US-guided needle biopsy becomes more important, useful, and valuable ( ).
For the evaluation of vessel signals in normal tissues, organs, and pathologic lesions, color Doppler US (CDUS) and Power Doppler US (PDUS) have been used to assess vessel signals, including those of the cardiovascular system, abdominal lesions, obstetric and gynecologic lesions, breast lesions, carotid and intracranial vessels, and pulmonary lesions ( ). Nevertheless, CDUS and PDUS can easily produce blooming effects of vessels and color noises in demonstrating the lesions abutting pulsatile organs ( ). The blooming effects of vessels render the US assessment of vessel signals not so real, and color noises lower confidence in the US demonstration of vessel signals.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Chest US Examinations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Definition of Vessel Signal, Blooming Effect and Color Noise of Sonographic Appearances
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Data Interpretation, Comparison, and Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Demographic Data
Get Radiology Tree app to read full this article<
Table 1
Demographic Data and Clinical Diagnoses in 34 Patients with Thoracic Lesions
Items Number ( n ) Patient no. 34 Sex (M/F) 28/6 Age (Mean ± SD) 58.6 ± 16.9 (23–86) Clinical diagnoses Lung cancer 18 Squamous cell carcinoma 11 Adenocarcinoma 5 Small-cell lung cancer 2 Metastatic colon cancer 1 Metastatic breast cancer 1 Anterior mediastinal tumor 4 Thymoma 1 Malignant lymphoma 2 Germ cell tumor 1 Benign lesions 9 Tuberculosis 4 Lung abscess 2 Pneumonia 3 Unknown diagnosis 1
Table 2
Lesion Sizes, Locations, and Abutting Pulsatile Organs in 34 Thoracic Lesions
Items Number ( n ) Locations Left upper lobe 15 Right upper lobe 9 Left lower lobe 3 Right middle lobe 3 Anterior mediastinum 4 Lesion size <5 cm 2 5–10 cm 21 10–15 cm 9 ≥15 cm 2 Abutting pulsatile organ Heart 13 Aorta 14 Pulmonary artery 7
Get Radiology Tree app to read full this article<
Comparison of Vessel Signals, Blooming Effect, Color Noises, and Influence of Needle Biopsy Decision between Different US Modes
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Imaging Quality Comparison between DFUS, CDUS, and PDUS in 34 Thoracic Lesions
US Mode Imaging Quality DFUS n (%) CDUS n (%) PDUS n (%) Vessel Signals Clear 31 (91) 31 (91) 29 (85) Cloudy 3 (9) 1.00 ⁎ ‡ 3 (9) 0.71 ⁎ § 5 (15) 0.71 ⁎ ∥ Blooming effect Prominent 0 (0) 22 (65) 25 (74) Acceptable 34 (100) <0.001 † ‡ 12 (35) 0.431 † § 9 (26) <0.001 † ∥ Color noise Prominent 1 (3) 11 (32) 21 (62) Acceptable 33 (97) 0.001 † ‡ 23 (68) 0.015 † § 13 (38) 0.001 † ∥ Needle biopsy Affect or change decision 1 (3) 0.003 † ‡ 10 (29) 0.442 † § 13 (38) No influence 33 (97) 24 (71) 21 (62) <0.001 † ∥
DFUS, dynamic flow ultrasound; CDUS, color Doppler ultrasound; PDUS, power Doppler ultrasound.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Illustrative Cases
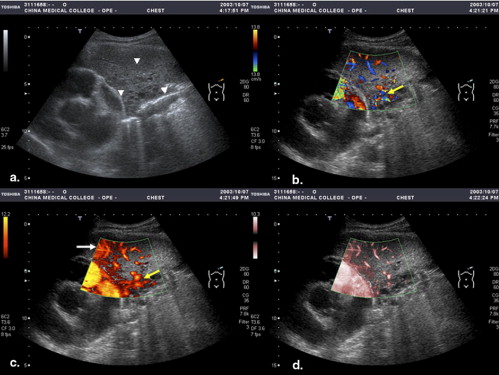
Patient 1
Get Radiology Tree app to read full this article<
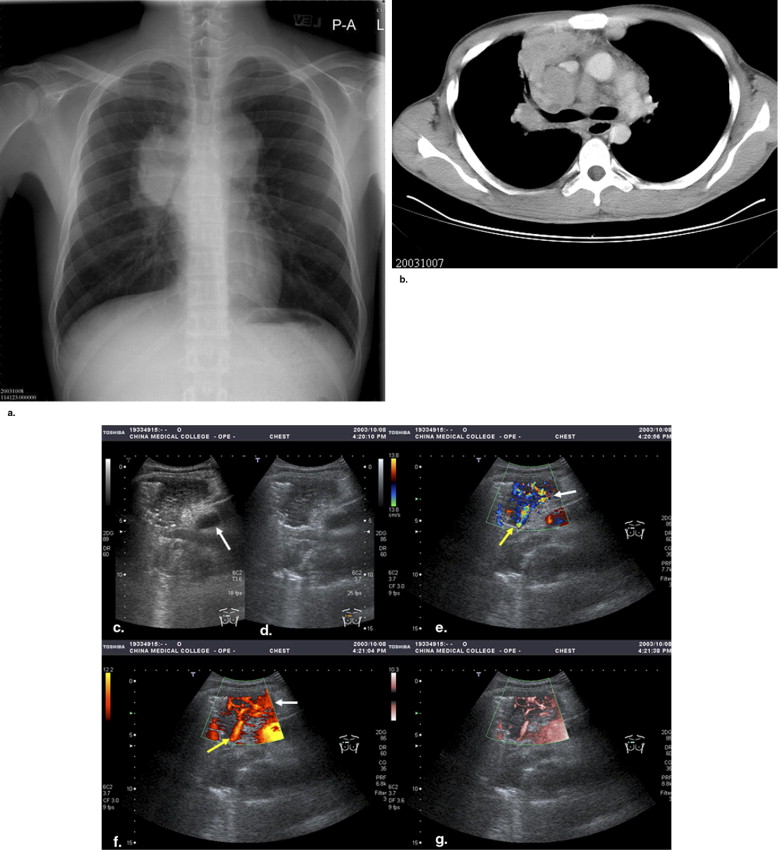
Get Radiology Tree app to read full this article<
Patient 2
Get Radiology Tree app to read full this article<
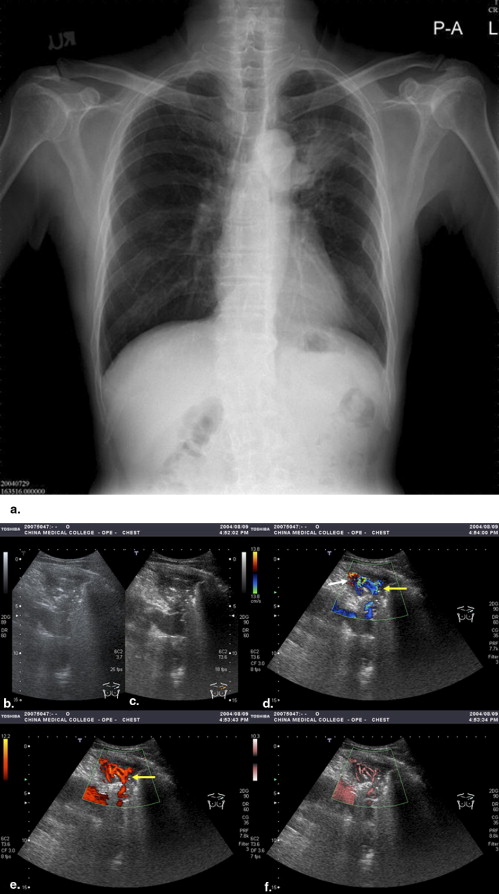
Get Radiology Tree app to read full this article<
Patient 3
Get Radiology Tree app to read full this article<
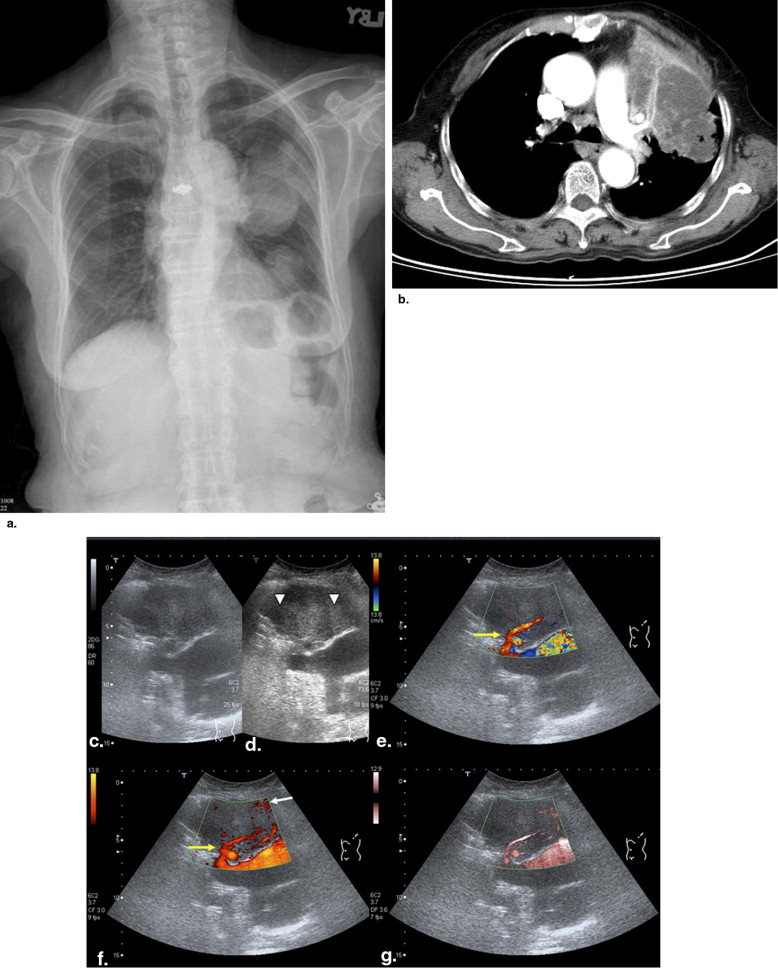
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Izumi S., Tamaki S., Natoli H., et. al.: Ultrasonically guided aspiration needle biopsy in diseases of the chest. Am Rev Respir Dis 1982; 125: pp. 460-464.
2. Sugama Y., Tamaki S., Kitamura S., et. al.: Ultrasonographic evaluation of pleura and chest wall invasion. Chest 1988; 93: pp. 275-279.
3. Ikezoe J., Morimoto S., Arizawa J., et. al.: Percutaneous biopsy of thoracic lesions: value of sonography for needle guidance. AJR Am J Roentgenol 1990; 154: pp. 1181-1185.
4. Yang P.C., Chang D.B., Yu C.J., et. al.: Ultrasound-guided core biopsy of thoracic tumors. Am Rev Respir Dis 1992; 146: pp. 763-767.
5. Yu C.J., Yang P.C., Chang D.B., et. al.: Diagnostic and therapeutic value of chest sonography: value in critically ill patients. AJR Am J Roentgenol 1992; 159: pp. 695-701.
6. Lichtenstein D., Hulot J.S., Rabiller A., et. al.: Feasibility and safety of ultrasound-aided thoracentesis in mechanically ventilated patients. Intensive Care Med 1999; 25: pp. 955-958.
7. Yang P.C., Luh K.T., Chang D.B., et. al.: Ultrasonographic evaluation of pulmonary consolidation. Am Rev Respir Dis 1992; 146: pp. 757-762.
8. Wang H.C., Yang P.C., Yu C.J., et. al.: Transthoracic needle biopsy of thoracic tumor by color Doppler ultrasound puncture guiding device. Thorax 1995; 50: pp. 1258-1263.
9. Yu C.J., Yang P.C., Chang D.B., et. al.: Evaluation of ultrasound-guided biopsies of mediastinal masses. Chest 1991; 100: pp. 399-405.
10. Gorguner M., Misirlioglu F., Polat P., et. al.: Color Doppler sonographically guided transthoracic needle aspiration of lung and mediastinal masses. J Ultrasound Med 2003; 22: pp. 703-708.
11. Hsu W.H., Chiang C.D., Chen C.Y., et. al.: Color Doppler ultrasound pulsatile flow signals of thoracic lesions: comparison of lung cancers and benign lesions. Ultrasound Med Biol 1998; 24: pp. 1087-1095.
12. Taylor K.J.W., Ramos I., Carter D., et. al.: Correlation of Doppler US tumor signals with neovascular morphologic features. Radiology 1988; 166: pp. 57-62.
13. Cosgrove D.O., Bamber J.C., Davey J.B., et. al.: Color Doppler signals from breast tumors. Radiology 1990; 176: pp. 175-180.
14. Tanaka S., Kitamura T., Fujita M., et. al.: Color Doppler flow imaging of liver tumors. Am J Roentgenol 1990; 154: pp. 509-514.
15. Wu C.C., Lee C.N., Chen T.M., et. al.: Incremental angiogenesis assessed by color Doppler ultrasound in the tumorigenesis of ovarian neoplasms. Cancer 1994; 73: pp. 1251-1256.
16. Foley W.D., Erickson S.J.: Color Doppler flow imaging. Am J Roentgenol 1991; 156: pp. 3-13.
17. Horstman W.G., Middleton W.D., Melson L.: Scrotal inflammatory disease: color Doppler US findings. Radiology 1991; 179: pp. 55-59.
18. Rubin J.M., Bude R.O., Carson P.L., et. al.: Power Doppler US: a potentially useful alternative to mean frequency-based color Doppler US. Radiology 1994; 190: pp. 853-856.
19. Bude R.O., Rubin J.M., Adler R.S.: Power versus conventional color Doppler sonography: comparison in the depiction of normal intrarenal vasculature. Radiology 1994; 192: pp. 777-780.
20. Hsu W.H., Ikezoe J., Chen C.Y., et. al.: Color Doppler ultrasound signals of thoracic lesions: comparison with resected histologic specimens. Am J Respir Crit Care Med 1996; 153: pp. 1938-1951.
21. Nilsson A.: Artifacts in sonography and Doppler. Eur Radiol 2001; 11: pp. 1308-1315.
22. Correas J.M., Bridal L., Lesavre A., et. al.: Ultrasound contrast agents: properties, principles of action, tolerance, and artifacts. Eur Radiol 2001; 11: pp. 1316-1328.
23. Gorg C., Seifart U., Gorg K., et. al.: Color Doppler sonographic mapping of pulmonary lesions: evidence of dual arterial supply by spectral analysis. J Ultrasound Med 2003; 22: pp. 1033-1039.
24. Sato T.: Technological description of dynamic flow. Toshiba Med Rev 2001; 25: pp. 29-33. (in Japanese)
25. Miyashita S.: Evaluation of the fetal circulation and veins. Toshiba Med Rev 2002; 56: pp. 750-756. (in Japanese)
26. Hotta N., Tagaya T., Maeno T.A., et. al.: Usefulness of contrast-enhanced ultrasonography with dynamic flow imaging to evaluate therapeutic effects for hepatocellular carcinoma. Hepatogastroenterology 2003; 50: pp. 1867-1871.
27. Hotta N., Tagaya T., Maeno T., et. al.: Advanced dynamic flow imaging with contrast-enhanced ultrasonography for the evaluation of tumor vascularity in liver tumors. J Clin Imag 2005; 29: pp. 34-41.