
Rationale and Objectives
The aim of this study was to prospectively evaluate the feasibility of a novel total liver volume perfusion computed tomographic technique in demonstrating treatment-site recurrence of liver metastases after radiofrequency ablation (RFA).
Materials and Methods
Eleven patients considered to be at increased risk for local RFA-site tumor recurrence underwent both positron emission tomography (PET) and perfusion computed tomography (CTP): a 12-phase scan of the entire liver acquired before and 11 times after contrast injection. After coregistration, blood flow maps were created using the maximum slope method.
Results
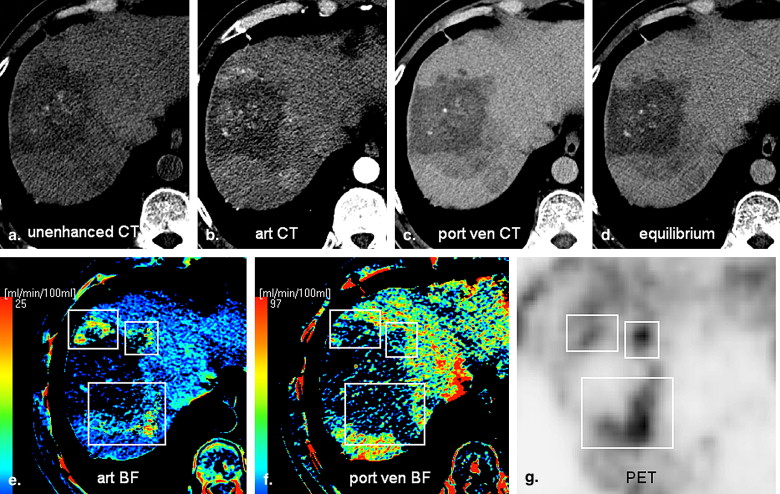
In all cases, the CTP-derived blood flow maps fully paralleled the PET images in showing either the absence (nine of 13 lesions) or presence (four of 13 lesions) of local RFA-site recurrence. Marginal lesions with high hepatic arterial perfusion (>50 mL/min/100 g) and low portal venous perfusion (<10 mL/min/100 g) represented recurring vital tumor tissue ( P < .05).
Conclusion
Total liver volume CTP seems feasible for the detection and localization of treatment-site recurrence after RFA.
Currently, the most widely used tumor ablative technique for the treatment of colorectal liver metastases (CRLMs) is radiofrequency ablation (RFA). In patients with unresectable hepatic tumors, RFA has proved to be safe and feasible . Furthermore, there are indications that RFA can improve both short-term and long-term survival . Unfortunately, up to 40% of treated patients have recurring disease, and 12% are found to have recurrence at a treatment site only 1 year after RFA ( ). If recurrence is limited to the treatment site, most often, a second RFA procedure or surgical resection can be performed.
At present, positron emission tomography (PET) is the best follow-up imaging modality for the early detection of recurrence, although PET cannot be used as an image-guiding technique for local ablative therapies such as RFA . However, PET combined with computed tomography (CT) can provide exact localization of active tumor tissue ( ), although this equipment is expensive and as yet not widely available. Using conventional CT, one study showed that of 38 ablated hepatocellular carcinomas that initially showed no enhancement, eight actually did recur. The authors concluded that short-term follow-up CT performed <3 months after treatment is not a reliable method to determine remission . Differentiation between vital tumor tissue and post-RFA necrosis with perilesional inflammation can be difficult if not impossible using CT or ultrasound. We evaluated the feasibility of a technique using total volume perfusion CT (CTP), combining morphologic and dynamic enhancement information from a multiphase computed tomographic scan with hemodynamic blood flow maps, for the detection of local treatment-site recurrence after RFA.
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Table 1
Results of PET and CTP for 13 Post-RFA Liver Lesions in 11 Patients for the Detection of Local RFA-Site Tumor Recurrence
CTP PET Center Rim Subject Lesion Primary Tumor Time After RFA (mo) Lesion Size (cm) Center Rim Arterial Portal Venous Arterial (mL/min/100 g) Portal Venous (mL/min/100 g) Histology 6-mo Follow-Up PET and CT Final Diagnosis 1 1 CRLM 6 4.0 − − − − = 18 = 69 No biopsy − No recurrence 2 2 CRLM 12 4.0 − − − − = 5 = 34 No biopsy − No recurrence 3 3 CRLM 12 4.2 − − − − = 14 = 102 No biopsy − No recurrence 4 4 CRLM 13 4.9 − − − − = 21 = 55 No biopsy − No recurrence 5 5 CRLM 6 3.5 − − − − = 9 = 60 No biopsy − No local recurrence ∗ 6 CRLM 6 5.5 − =/+ − − =/+ 31 = 44 No biopsy − Marginal inflammation 7 CRLM 6 4.0 − =/+ − − =/+ 62 = 28 No biopsy − Marginal inflammation 6 8 CRLM 8 4.8 − =/+ − − =/+ 29 = 12 No biopsy − Marginal inflammation 7 9 CRLM 7 5.4 − − − − =/+ 24 = 82 No biopsy − Reactive marginal hyperemia 8 10 ACUP 3 8.0 − + − − + 60 − <5 No biopsy + RFA-site recurrence 9 11 CRLM 9 5.0 − + − − + 140 − <5 + Repeat RFA RFA-site recurrence 10 12 CRLM 6 3.5 − + − − + 96 − <5 + Repeat RFA RFA-site recurrence 11 13 CRLM 6 5.7 − + − − + 105 − <5 + Repeat RFA RFA-site recurrence
ACUP, adenocarcinoma of unknown primary; CRLM, colorectal liver metastasis; CT, computed tomography; CTP, perfusion computed tomography; PET, positron emission tomography; RFA, radiofrequency ablation; −, decreased or absent tracer uptake or tissue blood flow compared to normal liver parenchyma; = , comparable tracer uptake or tissue blood flow compared to normal liver parenchyma; = /+, vaguely increased tissue blood flow compared to normal liver parenchyma; +, increased tracer uptake or tissue blood flow in at least focal spot.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Scanning Protocol and Image Postprocessing
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Results of PET
Get Radiology Tree app to read full this article<
Results of CTP
Get Radiology Tree app to read full this article<
Case 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 2
Get Radiology Tree app to read full this article<
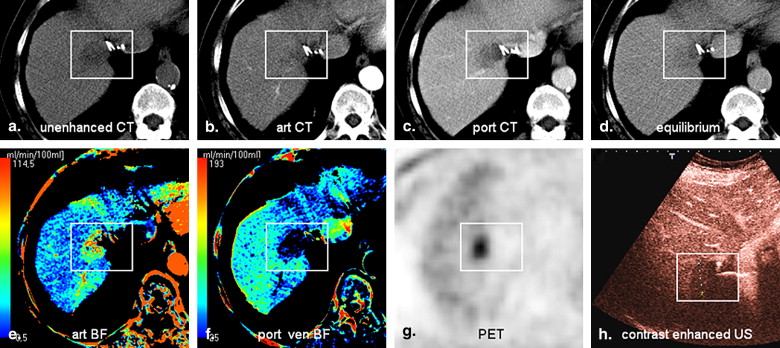
![Figure 2, Focal radiofrequency ablation (RFA)–site recurrence 9 months after the ablation of a large colorectal liver metastasis. Arterial (art) (a) and portal venous (port ven) (b) phase images on computed tomography (CT) with typical perilesional slightly increased hepatic artery blood flow (BF) (c) , normal portal venous blood flow (d) , and somewhat increased 2- [ 18 F]fluoro-2-deoxyglucose uptake on positron emission tomography (PET) (e) . This rim region probably represents reactive inflammatory tissue and should not be mistaken for tumor recurrence. In the same patient, a few centimeters caudally, a superficial focal spot that is hyperdense during the arterial phase (f) and isodense during the portal venous phase (g) is shown. This spot has a very high hepatic artery blood flow (h) and absent portal venous blood flow (i) , which clearly parallels the PET-positive focus (j) . A core biopsy proved the presence of tumor recurrence.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/EarlyDetectionofLocalRFASiteRecurrenceUsingTotalLiverVolumePerfusionCT/1_1s20S107663320900258X.jpg)
Get Radiology Tree app to read full this article<
Case 3
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantification
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Curley S.A., Izzo F., Delrio P., et. al.: Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg 1999; 230: pp. 1-8.
2. de Baere T.: Radiofrequency ablation of the liver. AJR Am J Roentgenol 2001; 177: pp. 1213-1215.
3. Leen E., Horgan P.G.: Radiofrequency ablation of colorectal liver metastases. Surg Oncol 2007; 16: pp. 47-51.
4. Solbiati L., Livraghi T., Goldberg S.N., et. al.: Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology 2001; 221: pp. 159-166.
5. Scaife C.L., Curley S.A.: Complication, local recurrence, and survival rates after radiofrequency ablation for hepatic malignancies. Surg Oncol Clin N Am 2003; 12: pp. 243-255.
6. Abdalla E.K., Vauthey J.N., Ellis L.M., et. al.: Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann Surg 2004; 239: pp. 818-825.
7. Donckier V., Van Laethem J.L., Goldman S., et. al.: [F-18] fluorodeoxyglucose positron emission tomography as a tool for early recognition of incomplete tumor destruction after radiofrequency ablation for liver metastases. J Surg Oncol 2003; 84: pp. 215-223.
8. Veit P., Antoch G., Stergar H., Bockisch A., Forsting M., Kuehl H.: Detection of residual tumor after radiofrequency ablation of liver metastasis with dual-modality PET/CT: initial results. Eur Radiol 2006; 16: pp. 80-87.
9. Tsushima Y., Funabasama S., Aoki J., Sanada S., Endo K.: Quantitative perfusion map of malignant liver tumors, created from dynamic computed tomography data. Acad Radiol 2004; 11: pp. 215-223.
10. Miles K.A., Hayball M., Dixon A.K.: Colour perfusion imaging: a new application of computed tomography. Lancet 1991; 337: pp. 643-645.
11. Meijerink M.R., van Waesberghe J.H., van der Weide L., van den Tol P., Meijer S., van Kuijk C.: Total-liver-volume perfusion CT using 3-D image fusion to improve detection and characterization of liver metastases. Eur Radiol 2008; 18: pp. 2345-2354.
12. Tsushima Y., Funabasama S., Sanada S., Aoki J., Endo K.: Development of perfusion CT software for personal computers. Acad Radiol 2002; 9: pp. 922-926.
13. Leggett D.A., Kelley B.B., Bunce I.H., Miles K.A.: Colorectal cancer: diagnostic potential of CT measurements of hepatic perfusion and implications for contrast enhancement protocols. Radiology 1997; 205: pp. 716-720.
14. Miles K.A., Leggett D.A., Kelley B.B., Hayball M.P., Sinnatamby R., Bunce I.: In vivo assessment of neovascularization of liver metastases using perfusion CT. Br J Radiol 1998; 71: pp. 276-281.
15. Meijerink M.R., van Cruijsen H., Hoekman K., et. al.: The use of perfusion CT for the evaluation of therapy combining AZD2171 with gefitinib in cancer patients. Eur Radiol 2007; 17: pp. 1700-1713.