
Rationale and Objectives
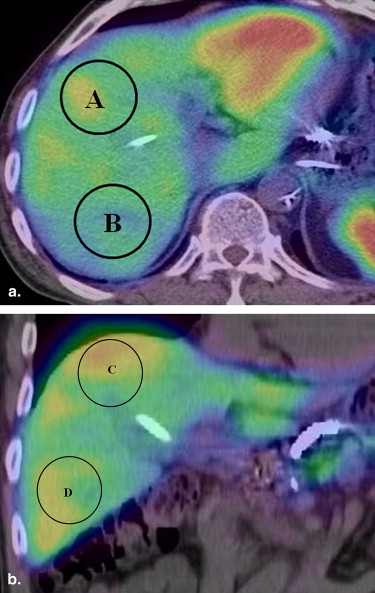
We evaluated the effect of gravity on intrahepatic perfusion (IHP) in patients with a port-catheter system (PCS) implanted for hepatic arterial infusion chemotherapy (HAIC). Using fused single photon-emission computed tomographic (SPECT)/computed tomographic (CT) images, we compared IHP after the injection of technetium-99m-labeled macroaggregated albumin (Tc-99m-MAA) via a PCS with the patient in the upright and decubitus positions.
Materials and Methods
We enrolled 27 patients with metastatic carcinoma of the liver who bore an implantable PCS for HAIC. SPECT/CT images were obtained on the third and seventh postimplantation day; 99mTc-MAA (185 MBq) was delivered with the patient in the upright and decubitus positions. We selected four regions of interest (ROIs) on SPECT images of the superior, inferior, anterior, and posterior regions. The anteroposterior and the superoinferior perfusion ratio (AP ratio, SI ratio) were derived from the mean counts in each ROI. Using an unpaired t -test, we compared these ratios after drug delivery in the upright and decubitus injection positions. We also visually compared IHP and classified the distribution of drugs delivered in the upright and decubitus positions on fused images. Moreover, using World Health Organization criteria, we evaluated the therapeutic response by comparing the tumor size on contrast-enhanced CT images obtained before and 3 months after treatment.
Results
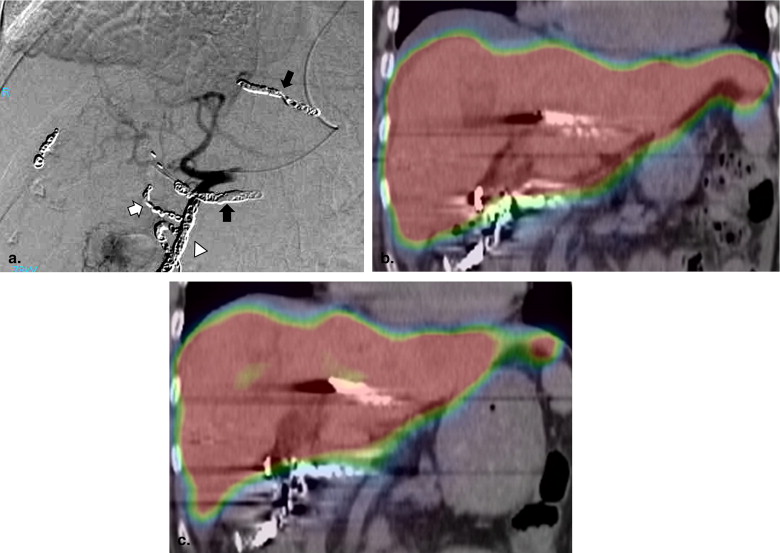
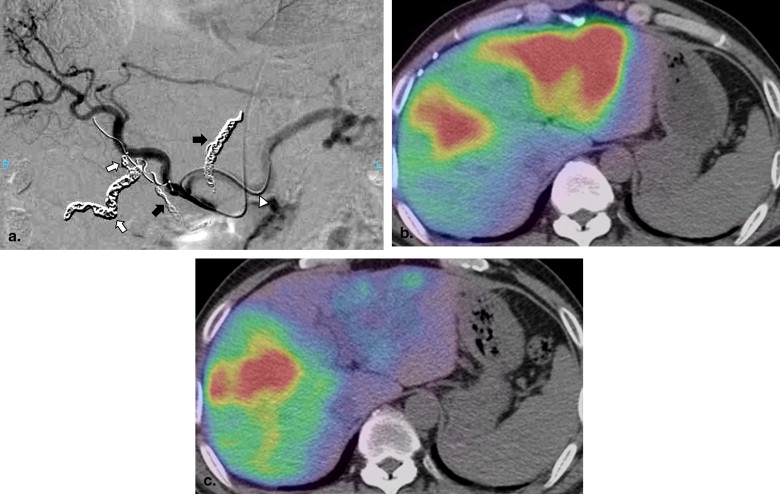
The SI ratios in the upright and decubitus injection positions were 1.14 and 0.92, respectively; the corresponding AP ratios were 1.47 and 1.73, respectively, indicating that there was no significant difference in these parameters irrespective of the injection position (SI ratio: P = .27, AP ratio: P = .35). However, in 14 of the 27 patients (52%), the visual appearance of IHP was different in the upright and decubitus positions. A change in the location of the catheter side hole when the decubitus was changed to the upright position produced a difference in IHP. Of 13 patients with identical drug distribution in both injection positions, six (46%) manifested a partial response (PR), five (38%) experienced no change (NC), and two (15%) experienced progressive disease (PD). Among the 14 patients with different drug distribution in the two injection positions, four (28%) achieved PR, five (36%) manifested NC, and the other five (36%) had PD.
Conclusions
Although the patient posture affected IHP by changing the position of the infusion catheter side hole in the liver, gravity had no significant effect on IHP in patients bearing an implantable PCS for the delivery of HAIC.
Hepatic arterial infusion chemotherapy (HAIC) via an implantable port-catheter system (PCS) is now used as a regional treatment for malignant tumors of the liver . We previously reported that fusion imaging using the combined single photon-emission computed tomographic (SPECT)/computed tomographic (CT) system reflects the actual distribution of the infused anticancer agent and that a good response requires direct perfusion of the area of malignancy . All patients in the earlier studies underwent abdominal SPECT with technetium-99m-labeled macroaggregated albumin (Tc-99m-MAA) delivered via the implantable port. 5-Fluorouracil (5-FU) was delivered via the arterial port for 5 or more hours and the posture of the patients was changed during HAIC.
According to Lisbona and colleagues , gravity had an effect on pulmonary perfusion scintigraphy with Tc-99m-MAA. In normal erect subjects, the flow of blood to the lungs from the pulmonary artery is strikingly nonuniform and West and colleagues documented that gravity strongly influences regional resistance via its effects on the capillary caliber.
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Port System Implantation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Fusion Images Using a Combined SPECT/CT System
Get Radiology Tree app to read full this article<
Drug Administration
Get Radiology Tree app to read full this article<
Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Comparison of SI and AP Ratios between Upright Injection and Decubitus Injection Perfusion Ratio (mean ± SD)
SI Ratio AP Ratio Upright injection 1.47 ± 0.21 ∗ 1.14 ± 0.17 ∗ † Decubitus injection 1.73 ± 0.19 ∗ 0.92 ± 0.08 ∗
AP, anteroposterior; SD, standard deviation; SI, superoinferior;
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Difference in Intrahepatic Perfusion between Upright and Decubitus Injection in 2 Access Routes
Identical Distribution Different Distribution Subclavian artery 12 8 Femoral artery 1 6
P = .04.
Table 3
Difference in Intrahepatic Perfusion between Upright and Decubitus Injection in 3 Groups
Identical Distribution Different Distribution Group 1 8 5 Group 2 2 4 Group 3 3 5
P = .29.
Intrahepatic perfusion patterns on fusion imaging in upright and decubitus positions. Group 1: the catheter was fixed in the gastroduodenal artery; Group 2: the catheter was fixed in a branch of the hepatic artery; Group 3: the catheter was placed in the splenic artery.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Relationship between Intrahepatic Perfusion Pattern on Fused Images and Initial Response of Liver Tumors
Initial Therapeutic Response Fused Image CR PR NC PD Identical drug distribution — 6 5 2 Different drug distribution — 4 5 5
CR, complete response; NC, no change; PD, progressive disease; PR, partial response.
P = .57.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Arai Y.: Interventional radiology for hepatic arterial infusion chemotherapy. Gan To Kagaku Ryoho 1996; 23: pp. 1385-1389.
2. Ensminger W., Niederhuber J., Dakhil S., et. al.: Totally implanted drug delivery system for hepatic arterial chemotherapy. Cancer Treat Rep 1981; 65: pp. 393-400.
3. Barone R.M., Byfield J.E., Goldfarb P.B., et. al.: Intraarterial chemotherapy using an implantable infusion pump and liver irradiation for the treatment of hepatic metastases. Cancer 1982; 50: pp. 850-862.
4. Ikeda O., Kusunoki S., Nakaura T., et. al.: Comparison of fusion imaging using a combined SPECT/CT system and intra-arterial CT: assessment of drug distribution by an implantable port system in patients undergoing hepatic arterial infusion chemotherapy. Cardiovasc Intervent Radiol 2006; 29: pp. 371-379.
5. Ikeda O., Tamura Y., Nakanone Y., et. al.: Evaluation of extrahepatic perfusion of anticancer drugs in the right gastric arterial region on fusion images using combined CT/SPECT: is extrahepatic perfusion predictive of gastric toxicity?. Cardiovasc Intervent Radiol 2007; 30: pp. 392-397.
6. Ikeda O., Tamura Y., Nakanone Y., et. al.: Evaluation of intrahepatic perfusion on fusion images using a CT/SPECT combined system: influence of anatomic variations on hemodynamic modification before installation of implantable port systems for hepatic arterial infusion chemotherapy. Cardiovasc Intervent Radiol 2007; 30: pp. 383-391.
7. Ikeda O., Tamura Y., Nakasone Y., et. al.: Comparison of intrahepatic and pancreatic perfusion on fusion images using a combined SPECT/CT system and assessment of efficacy of combined continuous arterial infusion and systemic chemotherapy in advanced pancreatic carcinoma. Cardiovasc Intervent Radiol 2007; 30: pp. 912-921.
8. Lisbona R., Dean G.W., Hakim T.S.: Observations with SPECT on the normal regional distribution of pulmonary blood flow in gravity independent planes. J Nucl Med 1987; 28: pp. 1758-1762.
9. Anthonisen N.R., Milic-Emili J.: Distribution of pulmonary perfusion in erect man. J Appl Physiol 1966; 21: pp. 760-766.
10. Hughes J.M.B., Glazier J.B., Maloney J.E., et. al.: Effect of lung volume on the distribution of pulmonary blood flow in man. Respir Physiol 1968; 4: pp. 58-72.
11. West J.B., Dollery C.T., Naimark A.: Distribution of blood flow in isolated lungs. Relation to vascular and alveolar pressures. J Appl Physiol 1964; 19: pp. 713-724.
12. Lorenz M., Muller H.H.: Randomized, multicenter trial of fluorouracil plus leucovorin administered either via hepatic arterial or intravenous infusion versus fluorodeoxyuridine administered via hepatic arterial infusion in patients with nonresectable liver metastases from colorectal carcinoma. J Clin Oncol 2000; 18: pp. 243-254.
13. Allen-Mersh T.G., Earlam S., Fordy C., et. al.: Quality of life and survival with continuous hepatic-artery floxuridine infusion for colorectal liver metastasis. Lancet 1994; 344: pp. 1255-1260.
14. Permuti S., Bromberger-Barnea B., Bane H.N.: Alveolar pressure, pulmonary venous pressure and vascular waterfall. Med Thorac 1962; 19: pp. 239-260.