
Rationale and Objectives
Cardiac computed tomography (CT) has been used extensively to measure coronary artery calcification. However, extracoronary calcifications, such as aortic valve calcification (AVC), may have independent clinical significance as well. The ability to track calcification is dependent on the reproducibility of the original measurement, and the variability of extracoronary calcification measurements still is unknown. Accurate quantification of calcification of the aortic valve, mitral annulus (MAC), and thoracic aortic (TAC) may be possible by using cardiac CT.
Methods
A total of 1,729 randomly chosen participants (ages 45–84, 53% female, 28% African-American, 36% Caucasian, 11% Chinese, 25% Hispanic) of the Multi-Ethnic Study of Atherosclerosis underwent dual scanning by electron beam CT (EBT) or multidetector CT (MDCT) to assess coronary and extra-coronary calcifications. Two calcium measurement methods—Agatston score (AS) and volume score (VS)—were measured for each scan. Concordance for calcium positivity was assessed among all scans. Mean absolute and relative differences between calcium measures on scans 1 and 2, excluding cases for which both scans had a measure of zero, was modeled by using linear regression to compare variability between scanner types. A repeated measures analysis of variance test was used to compare variability across calcium measures, with mean percentage absolute difference as the outcome measure.
Results
Concordances for the presence of calcium between duplicate scans were high and similar for both EBT and MDCT. Concordance was high for all three extracoronary measures, with a kappa statistic of κ = 0.94–0.96. For all three extracoronary sites, Bland-Altman plots demonstrated excellent agreement, with almost all measures falling within the boundaries of the 95% confidence limits of reproducibility. AVC interscan variability was approximately 8% for both AS and VS, with improved variability for EBT as compared with MDCT. Mitral annular calcification demonstrated slightly lower variability than AVC for both scanner types (approximately 6%), with no significant differences between MDCT and EBT. Of the three extracoronary sites, TAC had the highest variability (10%), with MDCT variability slightly lower than EBT variability (9.3 vs. 10.2%, respectively, P = NS). Agatson and volume scores for each of the three extracoronary sites were similar.
Conclusions
Overall rescan measurement variabilities for extracoronary calcification are low and should not be an impediment to the use of this test for studying progression of extracoronary calcification over time.
Atherosclerosis is a systemic process with a predilection for certain anatomic locations. Emerging evidence indicates that calcifications in valvular and thoracic aorta are manifestations of generalized atherosclerosis ( ). Population-based studies have shown that aortic sclerosis and atherosclerosis share similar risk factors ( ).
Large studies have demonstrated computed tomography (CT) scanning to be a highly reproducible method for quantifying coronary artery calcification ( ), whereas smaller studies also have demonstrated excellent reproducibility of this technique for quantifying aortic valve calcification (AVC) ( ). However, no large studies have characterized the reproducibility of CT scanning for quantifying calcification of the thoracic aorta (TAC) or the mitral annulus (MAC). Also, no previous studies have compared the reproducibilities of two CT technologies, electron beam computed tomography (EBT), and multidetector computed tomography (MDCT) for quantifying AVC, TAC, and MAC. Because establishing measurement reproducibility is a necessary condition for following progression of calcification over time, demonstration of measurement reproducibility is an important step toward the eventual use of CT scanning for monitoring progression.
Get Radiology Tree app to read full this article<
Methods
Study Population
Get Radiology Tree app to read full this article<
CT Techniques
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Agreement of Extracoronary Measures for Presence of Calcium Between Scans 1 and 2 by Scanner Type
EBT ( n = 972) MDCT ( n = 757) Scan 1 Calcium = 0 Scan 1 Calcium >0 κ (95% CI) Scan 1 Calcium = 0 Scan 1 Calcium >0 κ (95% CI) AVC Scan 2 Calcium = 0 821 (85%) 3 (0.3%) κ = 0.97 (0.95–0.99) 633 (84%) 8 (1%) κ =0.91 (0.87–0.95) Scan 2 Calcium >0 5 (0.5%) 143 (15%) 10 (1%) 106 (14%) MAC Scan 2 Calcium = 0 849 (87%) 3 (0.3%) κ = 0.96 (0.93–0.98) 650 (86%) 2 (0.3%) κ = 0.95 (0.92–0.98) Scan 2 Calcium >0 5 (0.5%) 114 (12%) 7 (0.9%) 97 (13%) TAC Scan 2 Calcium = 0 636 (65%) 13 (1%) κ = 0.94 (0.91–0.96) 470 (62%) 6 (1%) κ = 0.97 (0.95–0.99) Scan 2 Calcium >0 14 (1%) 309 (32%) 5 (1%) 276 (37%)
κ: kappa statistic; CI: confidence interval; EBT: electron beam computed tomography; MDCT: multidetector computed tomography; AVC: aortic valve calcification; MAC: mitral annulus calcification; TAC: thoracic aorta calcification.
Table 2
Mean Absolute Rescan Difference for Extracoronary Calcium Measures by Scanner Type
Calcium Measure Mean Absolute Rescan Difference ⁎ Among Those With Both Scans >0 EBT MDCT_P_ Value AVC_n_ 151 124 Agatston score (95% CI) 11.08 (9.34–13.14) 11.68 (9.67–14.11) .685 Volume score (95% CI) 9.98 (8.46–11.79) 11.02 (9.18–13.25) .433 MAC_n_ 122 106 Agatston score (95% CI) 14.95 (12.10–18.47) 17.32 (13.80–21.73) .352 Volume score (95% CI) 12.01 (9.74–14.81) 17.87 (14.27–22.35) .012 TAC_n_ 336 287 Agatston score (95% CI) 20.68 (18.27–23.41) 16.58 (14.48–18.97) .019 Volume score (95% CI) 16.68 (14.69–18.93) 13.08 (11.39–15.01) .011
CI: confidence interval; EBT: electron beam computed tomography; MDCT: multidetector computed tomography; AVC: aortic valve calcification; MAC: mitral annulus calcification; TAC: thoracic aorta calcification.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
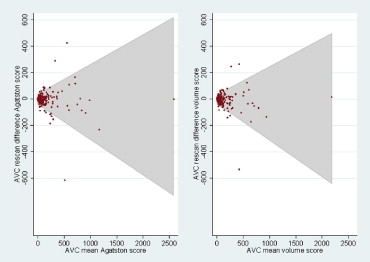
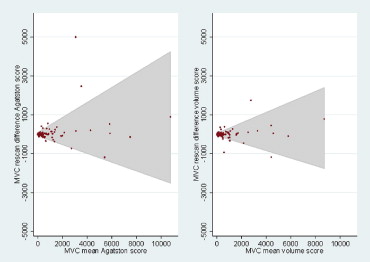
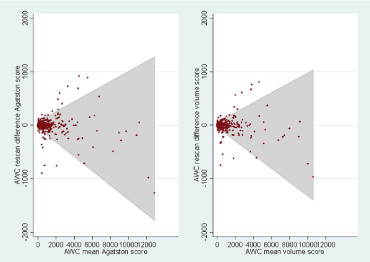
Table 3
Mean Relative Rescan Differences and Coefficients of Reproducibility for Each Scanner Type
Agatston Score (%) Volume Score (%)P Value (Agatston vs Volume Score) AVC EBT 6.8 6.1 .572 MDCT 9.9 9.7 .886 Both 8.1 7.7 .644 Reproducibility coefficient 0.295 0.298 NA MAC EBT 5.4 4.9 .624 MDCT 6.3 6.8 .697 Both 5.8 5.7 .949 Reproducibility coefficient 0.354 0.271 NA TAC EBT 11.3 10.3 .565 MDCT 8.9 8.0 .562 Both 10.2 9.3 .422 Reproducibility coefficient 0.140 0.135 NA
AVC: aortic valve calcification; EBT: electron beam computed tomography; MDCT: multidetector computed tomography; MAC: mitral annulus calcification; TAC: thoracic aorta calcification.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Agreement of Extracoronary Measures for Presence of Calcium Between Scans 1 and 2 ( n = 1729)
Scan 1 Calcium = 0 Scan 1 Calcium >0 κ\* (95% CI) AVC Scan 2 calcium = 0 1454 (84.1%) 11 (0.6%) κ = 0.94 (0.92–0.96) Scan 2 calcium >0 15 (0.9%) 249 (14.4%) MAC Scan 2 calcium = 0 1499 (86.8%) 5 (0.3%) κ = 0.96 (0.93–0.98) Scan 2 calcium >0 12 (0.7%) 211 (12.2%) TAC Scan 2 calcium = 0 1106 (64.0%) 19 (1.1%) κ = 0.95 (0.94–0.97) Scan 2 calcium >0 19 (1.1%) 585 (33.8%)
κ: kappa statistic; CI: confidence interval; AVC: aortic valve calcification; MAC: mitral annulus calcification; TAC: thoracic aorta calcification.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Budoff M.J., Takasu J., Katz R., et. al.: Reproducibility of CT measurements of aortic valve calcification, mitral annulus calcification, and aortic wall calcification in the multi-ethnic study of atherosclerosis. Acad Radiol 2006; 13: pp. 166-172.
2. Adler Y., Fisman E.Z., Shemesh J., et. al.: Spiral computed tomography evidence of close correlation between coronary and thoracic aorta calcifications. Atherosclerosis 2004; 176: pp. 133-138.
3. Allison M.A., Cheung P., Criqui M.H., et. al.: Mitral and aortic annular calcification are highly associated with systemic calcified atherosclerosis. Circulation 2006; 113: pp. 861-866.
4. Pohle K., Otte M., Maffert R., et. al.: Association of cardiovascular risk factors to aortic valve calcification as quantified by electron beam computed tomography. Mayo Clin Proc 2004; 79: pp. 1242-1246.
5. Yamamoto H., Shavelle D., Takasu J., et. al.: Valvular and thoracic aortic calcium as a marker of the extent and severity of angiographic coronary artery disease. Am Heart J 2003; 146: pp. 153-159.
6. Wong N.D., Sciammarella M., Arad Y., et. al.: Relation of thoracic aortic and aortic valve calcium to coronary artery calcium and risk assessment. Am J Cardiol 2003; 92: pp. 951-955.
7. Stewart B.F., Siscovick D., Lind B.K., et. al.: Clinical factors associated with calcific aortic valve disease: Cardiovascular Health Study. J Am Coll Cardiol 1997; 29: pp. 630-634.
8. Boon A., Cheriex E., Lodder J., et. al.: Cardiac valve calcification: characteristics of patients with calcification of the mitral annulus or aortic valve. Heart 1997; 78: pp. 472-474.
9. Mao S.S., Bakhsheshi H., Lu B., et. al.: Effect of ECG triggering on reproducibility of coronary artery calcium scoring. Radiology 2001; 220: pp. 707-711.
10. Kizer J.R., Gefter W.B., deLemos A.S., et. al.: Electron beam computed tomography for the quantification of aortic valvular calcification. J Heart Valve Dis 2001; 10: pp. 361-366.
11. Bild D.E., Bluemke D.A., Burke G.L., et. al.: Multi-Ethnic Study of Atherosclerosis: objectives and design. Am J Epidemiol 2002; 156: pp. 871-881.
12. Carr J.J., Nelson J.C., Wong N.D., et. al.: Calcified coronary artery plaque measurement with cardiac CT in population-based studies: standardized protocol of Multi-Ethnic Study of Atherosclerosis (MESA) and Coronary Artery Risk Development in Young Adults (CARDIA) study. Radiology 2005; 234: pp. 35-43.
13. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
14. Callister T.Q., Cooil B., Raya S.P., et. al.: Coronary artery disease: improved reproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology 1998; 208: pp. 807-814.
15. Shavelle D.M., Budoff M.J., Buljubasic N., et. al.: Usefulness of aortic valve calcium scores by electron beam computed tomography as a marker for aortic stenosis. Am J Cardiol 2003; 92: pp. 349-353.
16. Detrano R.C., Anderson M., Nelson J., et. al.: Coronary calcium measurement: effect of CT scanner type and calcium measure on the rescan reproducibility-MESA study. Radiology 2005; 236: pp. 477-484.
17. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography, a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
18. Shavelle D.M., Takasu J., Budoff M.J., et. al.: HMG CoA reductase inhibitor (statin) and aortic valve calcium. Lancet 2002; 359: pp. 1125-1126.
19. Otto C.M., Lind B.K., Kitzman D.W., et. al., Cardiovascular Health Study: Association of Aortic-Valve Sclerosis with Cardiovascular Mortality and Morbidity in the Elderly. N Engl J Med 1999; 341: pp. 142-147.