
Rationale and Objectives
To review sustainability and fair access related to setting up a centralized transient elastography (TE) program in the radiology department and to perform a quality assessment of a novel liver fibrosis evaluation program that combines TE with limited abdominal ultrasound (US).
Material and Methods
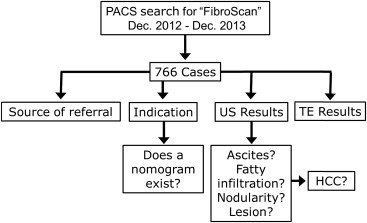
As part of a quality assessment, a retrospective chart review was performed on 758 patients who underwent TE immediately after limited abdominal US of the liver over a 12-month period. The elastography results and sonographic findings were documented, including the number and type of lesions identified. In terms of fair access evaluation, the indication for TE and referring service was reviewed for each case.
Results
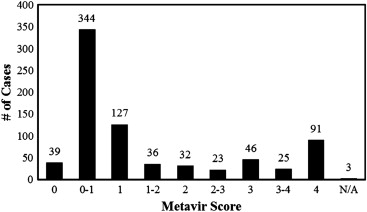
Most referrals were initiated by infectious disease (52.2% [396 of 758]) or gastroenterology (46.3% [351 of 758]) for patients with viral hepatitis (29.8% [226 of 758] for HBV and 52.2% [396 of 758] for HCV) and nonalcoholic steatohepatitis (11.9% [90 of 758]). Only 3.2% (24 of 758) of indications were outside the usual indications for which standardized values of TE were available. Most studies demonstrated minimal fibrosis (66.6% [510 of 766] ≤F1) or more advanced fibrosis (21.1% [162 of 766] ≥F3). Liver nodularity was observed in 63 cases, correlating to F2 fibrosis and above in 81.0% (51 of 63). US screening detected five new cases of hepatocellular carcinoma (HCC).
Conclusions
This unique program allows fair access and ensures that referrals are requested for appropriate indications. Concurrent US confers many advantages including proper TE probe placement to optimize measurement success, characterization of sonographic features that correlate with advanced fibrosis, and provides an opportunity to screen for HCC, in a population which may not otherwise have access to standardized screening.
Transient elastography (TE, FibroScan; Echosens, Paris, France) is a noninvasive modality that measures liver stiffness by determining the velocity of a shear wave produced by mechanical stress as it propagates through tissue. The measurement is recorded in kilopascal, and then, a Metavir score (F0–F4) is assigned on the basis of standard values developed for specific liver pathology . Biopsy is often considered the gold standard for assessing liver fibrosis; however, it is prone to sampling error and interobserver variability among pathologists . There is also a risk of complications for patients including bleeding, infection, damage to adjacent structures, and, rarely, death . TE circumvents these limitations as it is noninvasive and surveys a volume of tissue that is 100 times that of biopsy, thereby reducing sampling error . It has been extensively compared to biopsy for diagnostic accuracy and is regarded as a suitable alternative for assessing fibrosis . In particular, it is effective at distinguishing cirrhosis from normal liver tissue but correlates less well to histology when there are intermediate stages of fibrosis . Although TE is straightforward to perform, it can be difficult to interrogate patients with large waist circumferences or narrow intercostal spaces, and the reliability of the results is dependent on the experience of the operator . Obesity also leads to liver stiffness measurement failure as adipose tissue attenuates the shear wave. To overcome this, modified probes have been developed for use in this population of patients . Because of normal anatomic variations and lack of real-time image guidance, other structures may be interposed between the right lower chest wall and the liver, including the colon, gallbladder, or unusually larger hepatic vessels, all of which will negatively affect the TE results. Finally, TE is limited to assessing liver stiffness in the context of specific disease for which cutoff values have been published, including hepatitis B, hepatitis C, HIV/hepatitis C co-infection , alcoholic hepatitis , and nonalcoholic steatohepatitis (NASH) . It is uncertain if these values can be applied to other etiologies of liver fibrosis.
Our hospital implemented a liver fibrosis evaluation program using TE. In an era of cost containment and rational use of resources, the TE unit was placed in the radiology department, a neutral location allowing for equitable access. The decision was also made to perform TE in combination with a limited abdominal B-mode ultrasound (US) of the liver before TE measurements in the same visit. The goal was to optimize TE measurements under US guidance and screen for evidence of liver disease. Performing US first ensures patients do not have ascites between the chest wall and the liver being interrogated, which will affect the accuracy of TE results. Specialized probes combining B-mode US and TE within the same unit have been shown to improve the efficiency and accuracy of measuring liver stiffness by assisting the operator select regions of interest to avoid large hepatic vessels under direct image guidance . Compared to these other systems, our program differs because a B-mode US of the liver was performed with a separate probe before TE to determine the optimal intercostal space for acquiring liver stiffness measurements. The images were also reviewed by a radiologist for assessment of evidence for liver pathology such as fatty infiltration, mass lesions, and cirrhotic changes. A significant advantage of this program is screening for possible hepatocellular carcinoma (HCC), which is particularly relevant for patients with hepatitis B or chronic hepatitis C with changes of fibrosis. In Canada and the United States, present guidelines recommend biyearly screening for HCC with sonography in patients with hepatitis B or frank cirrhosis of any cause .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Study Demographics
Variable Value (%) Patient demographics ( n = 758) Male 439 (57.9) Female 319 (42.1) Age (years ± standard deviation) 50.7 ± 11.6 Indication ( n = 758) Hepatitis C 396 (52.2) Hepatitis B 226 (29.8) Nonalcoholic steatohepatitis 90 (11.9) Hepatitis C/HIV co-infection 16 (2.1) Alcoholic hepatitis 6 (0.8) Indications without a nomogram 24 (3.2) Methotrexate-induced fibrosis 8 (1.1) Primary biliary cirrhosis 5 (0.7) Chronic liver disease 4 (0.5) Autoimmune hepatitis 3 (0.4) Wilson disease 2 (0.3) Hepatitis B/hepatitis C co-infection 1 (0.1) Hemachromocytosis 1 (0.1) Referring service ( n = 758) Infectious disease 396 (52.2) Gastroenterology 351 (46.3) Other 10 (1.3)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Ultrasound Results
Variable Value (%) Ascites 4 (—) Nodularity ( n = 63) ≥F2 Fibrosis 51 (81.0) Fatty infiltration ( n = 179) NASH 55 (30.7) Other (ie, viral hepatitis) 124 (69.3) Fatty sparing ( n = 23) NASH 11 (47.8) Liver lesions at time of FibroScan ( n = 135) Cysts 63 (46.6) Solid lesions 72 (53.3) Hemangioma 44 (32.6) HCC 4 (3.0) Other benign 24 (17.8) HCC on subsequent imaging 2 (—)
HCC, hepatocellular carcinoma; NASH, nonalcoholic steatohepatitis.
Table 3
Cases of Discordance Between Sonographic Descriptions and TE
Indication TE Results ∗ US Findings Prior Biopsy ∗ Repeat TE ∗ Nodular Surface Coarse Echotexture Caudate Enlargement HCV 0–1 + − − − 3 NASH 0 + − − − − HCV 1 + + − 4 − HBV 0–1 + + − − − HBV 1 + + − 0 − EtOH hepatitis 1 + + − − 1 HCV 1–2 + + − 1 − HBV 0–1 + + − − 0–1 HCV 1–2 + − − 1–2 − HBV 0–1 + + + − − HCV 0–1 + + − − −
HBV, hepatitis B virus; HCV, hepatitis C virus; NASH, nonalcoholic steatohepatitis; TE, transient elastography; US, ultrasound.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. de Ledinghen V., Vergniol J.: Transient elastography (FibroScan). Gastroentérologie Clin Biol 2008; 32: pp. 58-67.
2. Afdhal N.H., Nunes D.: Evaluation of liver fibrosis: a concise review. Am J Gastroenterol 2004; 99: pp. 1160-1174.
3. Thampanitchawong P., Piratvisuth T.: Liver biopsy: complications and risk factors. World J Gastroenterol 1999; 5: pp. 301-304.
4. Cohen E.B., Afdhal H.N.: Ultrasound-based hepatic elastography origins, limitations and applications. J Clin Gastroenterol 2010; 44: pp. 637-645.
5. Friedrich-Rust M., Ong M.-F., Martens S., et. al.: Performance of transient elastography for the staging of liver fibrosis: a meta analysis. Gastroenterology 2008; 134: pp. 960-974.
6. Sandrin L., Fourguet B., Hasquenoph J.-M., et. al.: Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol 2003; 29: pp. 1705-1713.
7. Castera L., Foucher J., Bernard P.-H., et. al.: Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatology 2010; 51: pp. 828-835.
8. Myers R.P., Pomier-Layrargues G., Kirsch R., et. al.: Discordance in fibrosis staging between liver biopsy and transient elastography using the FibroScan XL probe. J Hepatol 2012; 56: pp. 564-570.
9. de Ledinghen V., Wong V.W.-S., Vergniol J., et. al.: Diagnosis of liver fibrosis and cirrhosis using liver stiffness measurements: comparison between M and XL probe of FibroScan. J Hepatol 2012; 56: pp. 833-839.
10. Nguyen-Khac E., Chatelain D., Tramier B., et. al.: Assessment of asymptomatic liver fibrosis in alcoholic patients using fibroscan: prospective comparison with seven non-invasive laboratory tests. Aliment Pharmacol Ther 2008; 28: pp. 1188-1198.
11. Nahon P., Kattaneh A., Lemoine M.: Liver stiffness measurement in patients with cirrhosis and hepatocellular carcinoma: a case-control study. J Hepatol 2009; 49: pp. 1062-1068.
12. Yoneda M., Fujita K., Nakajima A., et. al.: Transient elastography in patients with non-alcoholic fatty liver disease (NAFLD). Gut 2007; 56: pp. 1330-1331.
13. Wong V.W., Vergniol J., Wong G.L.: Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease. Hepatology 2010; 51: pp. 454-464.
14. Mak T.M., Huang Y.P., Zheng Y.P.: Liver fibrosis assessment using transient elastography guided with real-time B-mode ultrasound imaging: a feasibility study. Ultrasound Med Biol 2013; 39: pp. 956-966.
15. Bruix J., Sherman M.: Management of hepatocellular carcinoma. Hepatology 2005; 42: pp. 1208-1236.
16. Sherman M., Burak K., Maroun J., et. al.: Multidisciplinary Canadian consensus recommendations for the management and treatment of hepatocellular carcinoma. Curr Oncol 2011; 18: pp. 228-324.
17. Talwalkar J.A., Kurtz D.M., Schoenleber S.J., et. al.: Ultrasound-based transient elastography for the detection of hepatic fibrosis: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2007; 5: pp. 1214-1220.
18. Gaia S., Carenzi S., Barilli A.L., et. al.: Reliability of transient elastography for the detection of fibrosis in non-alcoholic fatty liver disease and chronic viral hepatitis. J Hepatol 2011; 54: pp. 64-71.
19. Foucher J., Castera L., Bernard P.-H., et. al.: Prevalence and factors associated with failure of liver stiffness measurements using FibroScan in a prospective study of 2114 examinations. Eur J Gastroenterol Hepatol 2006; 18: pp. 411-412.
20. Ferraioli G., Parekh P., Levitov A., et. al.: Shear wave elastography for evaluation of liver fibrosis. J Ultrasound Med 2014; 33: pp. 197-203.
21. El-Serag H.B., Davila J.A.: Surveillance for hepatocellular carcinoma: in whom and how?. Ther Adv Gastroenterol 2011; 4: pp. 5-10.