
Rationale and Objectives
Splenic preservation is currently the trend for treatment of patients with splenic trauma to avoid complications of splenectomy. This study aimed to evaluate the feasibility of emergent transcatheter arterial embolization (TAE) for hemodynamically unstable patients with blunt splenic injury.
Materials and Methods
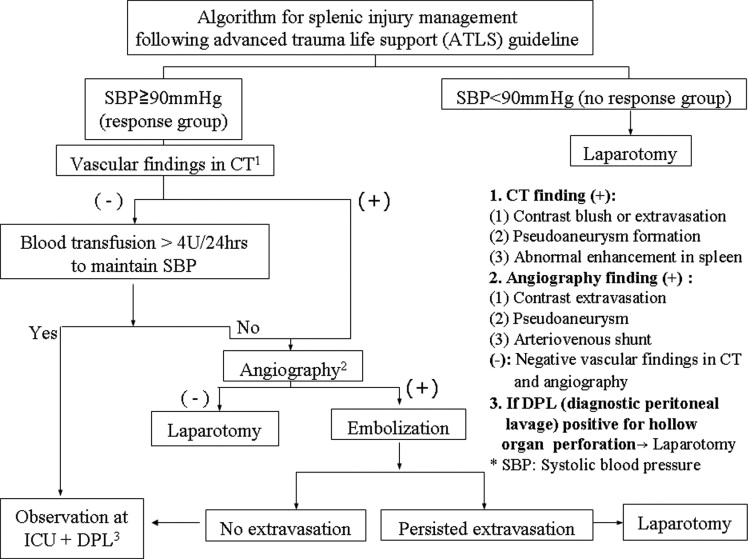
In a period of 2 years, 65 patients of blunt splenic trauma were studied. Patients with initial systolic blood pressure < 90 mmHg and showed initial response including rapid response and transient response to the emergent fluid resuscitation were included. Angiography and TAE was undertaken if contrast medium extravasation or pseudoaneurysm formation was noted in the computed tomography (CT) images, according to the criteria of American Association for the Surgery of Trauma. All patients who underwent TAE were admitted for observation of the possibility of delayed rupture.
Results
Thirteen hemodynamically unstable patients who were responsive to initial fluid resuscitation received angiography due to abnormal CT findings including contrast agent extravasation in 12 patients, 2 patients with arteriovenous fistula, and 8 patients with pseudoaneurysm formation. TAE was successfully performed in all of these 13 patients, including 2 patients with associated left renal injuries and 1 patient associated with bilateral internal mammary arteries injuries, without complications.
Conclusions
TAE is a safe and effective procedure for treating blunt splenic injury even in hemodynamically unstable patients who responded to initial fluid resuscitation.
Management of blunt splenic injuries has been changed from splenectomy toward splenic preservation such as use of hemostatic agents, suture of the laceration, partial splenectomy, and splenic reimplantation. Even so, these techniques may induce rebleeding or exacerbate bleeding from splenic injuries when the spleen was mobilized from its bed for remove all the blood clots from its surface.
Conservative treatment with bed rest and observation was used in pediatric patients of splenic injury with stable hemodynamic stable condition. When this was extended to the hemodynamic stable adult patients, it showed a relative high failure rate and hence is less encouraged ( ). Keramidas first reported successful splenic hemostasis by surgical ligation of the proximal splenic artery in 1979 ( ), and Sclafani et al had translated this concept into a percutaneous approach ( ). It was supposed that embolization of the proximal segment of main splenic artery would reduce the pressure in the spleen, help to heal the injury, and decrease the risk of secondary rupture of the spleen. After that, several similar studies with percutaneous transcatheter arterial embolization (TAE) were reported in effective control of bleeding for hemodynamically stable patients with blunt splenic injury and preserve the splenic function ( ), in contrast to the high failure rate of traditional nonoperative treatment of splenic injuries with strict bed rest and observation. The method of TAE in hemodynamic stable patients has shifted from embolization of the main trunk of the splenic artery to superselective embolization close to the bleeder. Although several reports proposed that embolization of the main trunk could preserve the splenic function by reperfusion via the collateral circulations but superselective embolization can reduce the infarction region to as small as possible.
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Imaging
Get Radiology Tree app to read full this article<
Table I
CT grading of splenic injuries according to the American Association for the Surgery of Trauma
Injury Grade Description of Injury Splenic hematoma I Subcapsular <10% surface area II Subcapsular 10–50% surface area; Parenchymal <5 cm in diameter III Subcapsular >50% surface area Ruptured subcapsular or parenchymal hematoma; Parenchymal >5 cm in diameter IV Parenchymal ruptured Splenic laceration I Capsular tear, <1 cm parenchymal depth II Capsular tear, 1–3 cm parenchymal depth that doesn’t involve a trabecular vessel III Parenchymal depth, >3 cm or involving trabecular vessels IV Laceration involving segmental or hilar vessels producing major devascularization (>25% of spleen) V Completely shattered spleen V/Vascular Hilar vascular injury that devascularizes spleen
Get Radiology Tree app to read full this article<
Angiography and TAE
Get Radiology Tree app to read full this article<
Post-TAE Care and Follow-up
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Godley C.D., Warren R.L., Sheridan R.L., et. al.: Nonoperative management of blunt splenic injury in adults: age over 55 years as a powerful indicator for failure. J Am Coll Surg 1996; 183: pp. 133-139.
2. Smith J.J., Cooney R., Mucha P.J.: Nonoperative management of the ruptured spleen: a revalidation of criteria. Surgery 1996; 120: pp. 745-750.
3. Keramidas D.C.: The ligation of the splenic artery in the treatment of traumatic rupture of the spleen. Surgery 1979; 85: pp. 530-533.
4. Sclafani S.J.A.: The role of angiographic hemostasis in salvage of the injured spleen. Radiology 1981; 141: pp. 645.
5. Hagiwara A., Yukioka T., Ohta S., et. al.: Nonsurgical management of patients with blunt splenic injury: efficacy of transcatheter arterial embolization. AJR Am J Roentgenol 1996; 167: pp. 159-166.
6. Wasvary H., Howells G., Villalba M., et. al.: Nonoperative management of adult blunt splenic trauma: a 15-year experience. Am Surg 1997; 63: pp. 694-699.
7. Wahl W.L., Ahrns K.S., Chen S., Hemmila M.R., Rowe S.A., Arbabi S.: Blunt splenic injury: operation versus angiographic embolization. Surgery 2004; 136: pp. 891-899.
8. Hagiwara A., Fukushima H., Murata A., et. al.: Blunt splenic injury: usefulness of transcatheter arterial embolization in patients with a transient response to fluid resuscitation. Radiology 2005; 235: pp. 57-64.
9. Bessoud B., Denys A., Calmes J.M., et. al.: Nonoperative management of traumatic splenic injuries: is there a role for proximal splenic artery embolization?. AJR Am J Roentgenol 2006; 186: pp. 779-785.
10. Killen K.L., Shanmuganathan K., Boyd-Kranis R., et. al.: CT findings after embolization for blunt splenic trauma. J Vasc Interv Radiol 2001; 12: pp. 209-214.
11. Sclafani S.J.A., Weisberg A., Scalea T.M., et. al.: Blunt splenic injuries: nonsurgical treatment with CT, angiography, and transcatheter arterial embolization of the splenic artery. Radiology 1991; 181: pp. 189-196.
12. Madoff D.C., Denys A., Wallace M.J., et. al.: Splenic arterial interventions: anatomy, indications, technical considerations, and potential complications. Radiographics 2005; 25: pp. S191-S211.
13. PeterEken A., McCarthy M.C., Woods R.J., et. al.: Complications arising from splenic embolization after blunt splenic trauma. Am Surg 2005; 189: pp. 335-339.