
Rationale and Objectives
Breast magnetic resonance imaging (MRI) is increasingly being added to mammography for screening asymptomatic women at increased risk of breast cancer. Because the direction and extent of correlation between mammography and MRI could potentially result in over- or underestimation of the diagnostic gain related to using MRI as an adjunct to mammographic screening, we performed an analysis to evaluate the extent of correlation between mammography and MRI.
Materials and Methods
We reviewed the published literature to identify multimodality breast cancer screening studies reporting the sensitivity of mammography and MRI, alone and in combination, for breast cancer diagnosis. After calculating the expected sensitivity of combined mammography and MRI under conditions of test independence (no correlation), we compared the calculated and observed sensitivities for combined mammography and MRI. We then calculated correlation coefficients for mammography and MRI.
Results
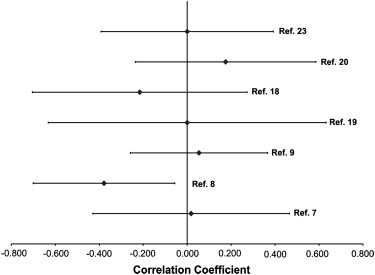
Seven studies of multimodality screening in women at increased risk of developing breast cancer were included for analysis. Of these studies, the correlation between film mammography and MRI was positive in three studies, negative in two studies, and not identified in two studies. The calculated correlation coefficients ranged from −0.38 to 0.18. In six of seven studies, the 95% confidence interval for the correlation coefficient included 0.0, indicating no significant correlation.
Conclusions
Evidence from published trials of multimodality breast cancer screening identified no statistically significant correlation between film mammography and MRI. Using both tests for breast cancer screening is likely to improve the early detection of breast cancer in women at increased risk.
Mammography is the current clinical standard for breast cancer screening. The accuracy of mammography in the general population is relatively high, with a meta-analysis of screening mammography reporting sensitivity in the range of 83%–95% and specificity of 94%–99% . However, the sensitivity of mammography in women at increased risk of breast cancer, including BRCA gene mutation carriers, is substantially lower, in the range of 33%–56% . This is thought to be related to multiple factors, such as the younger age at screening for these women, increased breast radiodensity, as well as pathologic and imaging characteristics of breast cancers in this population. Recent studies indicate that breast magnetic resonance imaging (MRI) is highly sensitive and can detect breast cancers not seen on mammography, particularly in women at increased risk . The American Cancer Society has endorsed the use of breast MRI as an adjunct to mammography for screening these women .
When two diagnostic tests are combined, a positive combined test can be defined in two ways: 1) either test with positive results is considered positive or 2) both tests with positive results are required for the combined test to be considered positive . In the published studies and in current clinical practice, a positive finding on either screening mammography or breast MRI is followed by further diagnostic evaluation. Thus the two-test combination is considered positive if either individual examination is positive.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Selection and Data Abstraction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Testing the Independence of Mammography and MRI
Get Radiology Tree app to read full this article<
Expected combined sensitivity=Sensitivity of Test1+(1−Sensitivity of Test1)∗(Sensitivity of Test2) Expected combined sensitivity
=
Sensitivity of Test
1
+
(
1
−
Sensitivity of Test
1
)
∗
(
Sensitivity of Test
2
)
For the studies included in this analysis, the expected sensitivity of the mammography and MRI combination, assuming statistical independence, was calculated and compared with the observed sensitivity of the two-test combination. Subsequently, using the observed sensitivities of mammography and MRI, alone and in combination, a correlation coefficient (ρ) was calculated to determine the direction and to quantify the magnitude of positive or negative correlation, as described by Shen et al (Sens Test 1 = sensitivity of the first test, Sens Test 2 = sensitivity of the second test, and Sens Observed Combination = observed sensitivity of the two test combination). For tests which are independent, the correlation coefficient is equal to zero.
ρ=Sens Test1+Sens Test2–(Sens Test1∗Sens Test2)–Sens Observed Combination(2)Sqrt [Sens Test1∗Sens Test2∗(1−Sens Test1)∗(1−Sens Test2)] ρ
=
Sens Test
1
+
Sens Test
2
–
(
Sens Test
1
∗
Sens Test
2
)
–
Sens Observed Combination
(
2
)
Sqrt [Sens Test
1
∗
Sens Test
2
∗
(
1
−
Sens Test
1
)
∗
(
1
−
Sens Test
2
)
]
The standard error for the correlation coefficient was also calculated .
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Summary of Studies included for Analysis
Study Warner et al Leach et al Kuhl et al Trecate et al Sardanelli et al Hagen et al Riedl et al Year published 2004 2005 2005 2006 2007 2007 2007 Study population BRCA1/2 carriers BRCA1/2, TP53 carriers Lifetime risk 20%, 21–40%, and mutation carriers BRCA1/2 carriers, first-degree relatives of carriers, or strong family history BRCA1/2 carriers, first-degree relatives of carriers, or strong family history BRCA1/2 carriers BRCA1/2 carriers, strong family history, or high risk based on Claus model No. women screened 236 649 529 116 278 491 327 No. cancers detected 22 35 43 12 18 25 28 Invasive 16 29 34 11 15 21 16 Ductal carcinoma in situ 6 6 9 1 3 4 12 No. screening rounds 3 5 5 1 2 3 6 Ave no. screens/patient 1.9 2.9 2.7 1.0 1.4 1.6 2.1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Mammography, MRI Sensitivity, and Correlation
Study Warner et al Leach et al Kuhl et al Trecate et al Sardanelli et al Hagen et al Riedl et al Positivity criterion BI-RADS 4,5 BI-RADS 0,3,4,5 BI-RADS 4,5 BI-RADS 4,5 BI-RADS 4,5 Norwegian scale value 3,4,5 BI-RADS 4,5 Mammography alone sensitivity 0.348 0.400 0.326 0.364 0.588 0.522 0.500 MRI alone Sensitivity 0.739 0.770 0.907 1.000 0.938 0.864 0.857 Combined (observed) sensitivity 0.826 0.940 0.93 1.000 1.000 0.905 0.929 Combined (calculated) Sensitivity 0.830 0.862 0.937 1.000 0.974 0.935 0.929 Correlation (direction) Positive Negative Positive Independent Negative Positive Independent Correlation coefficient (ρ) 0.018 −0.378 0.054 0.000 −0.216 0.175 0.000 Standard error 0.224 0.161 0.156 0.316 0.244 0.205 0.196
MRI, magnetic resonance imaging; BI-RADS, Breast Imaging Reporting and Data System .
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Mushlin A.I., Kouides R.W., Shapiro D.E.: Estimating the accuracy of screening mammography: a meta-analysis. Am J Prevent Med 1998; 14: pp. 143-153.
2. Brekelmans C.T.M., Seynaeve C., Bartels C.C.M., et. al.: Effectiveness of Breast cancer surveillance in BRCA 1/2 gene mutation carriers and women with high familial risk. J Clin Oncol 2001; 19: pp. 924-930.
3. Komenaka I.K., Ditkoff B., Joseph K., et. al.: The development of interval breast malignancies in patients with BRCA mutations. Cancer 2004; 100: pp. 2079-2083.
4. Meijers-Heijboer H., van Geel B., van Putten W.L.J., et. al.: Breast cancer after prophylactic bilateral mastectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med 2001; 345: pp. 159-164.
5. Scheuer L., Kauff N., Robson M., et. al.: Outcome of preventive surgery and screening for breast and ovarian cancer in BRCA mutation carriers. J Clin Oncol 2002; 20: pp. 1260-1268.
6. Kriege M., Brekelmans C.T.M., Boetes C., et. al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 2004; 351: pp. 427-437.
7. Warner E., Plewes D.B., Hill K.A., et. al.: Survillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004; 292: pp. 1317-1325.
8. Leach M.O., Boggis C.R., Dixon A.K., et. al.: Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 2005; 365: pp. 1769-1778.
9. Kuhl C.K., Schrading S., Leutner C.C., et. al.: Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 2005; 23: pp. 8469-8476.
10. Lehman C.D., Blume J.D., Weatherall P., et. al.: Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer 2005; 103: pp. 1898-1905.
11. Sardanelli F., Podo F.: Breast MR imaging in women at high-risk of breast cancer. Is something changing in early breast cancer detection?. Eur Radiol 2007; 17: pp. 873-887.
12. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society Guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clinicians 2007; 57: pp. 75-89.
13. Cebul R.D., Hershey J.C., Williams S.V.: Using multiple tests: Series and parallel approaches. Clin Lab Med 1982; 2: pp. 871-890.
14. Marshall R.J.: The predictive value of simple rules for combining two diagnostic tests. Biometrics 1989; 45: pp. 1213-1222.
15. Shen Y., Wu D., Zelen M.: Testing the independence of two diagnostic tests. Biometrics 2001; 57: pp. 1009-1017.
16. Rosner B.: Regression and correlation methods.5th ed2000.Duxbury Thomson LearningPacific Grove, CA
17. Lehman C.D., Issacs C., Schnall M.D., et. al.: Cancer yield of mammography, MRI, and US in high-risk women: prospective multi-institution breast cancer screening study. Radiology 2007; 244: pp. 381-388.
18. Sardanelli F., Podo F., D’Agnolo G., et. al.: Multicenter comparative multimodality surveillance of women at genetic-familial high-risk for breast cancer (HIBCRIT Study): interim results. Radiology 2007; 242: pp. 698-715.
19. Trecate G., Vergnaghi D., Manoukian S., et. al.: MRI in the early detection of breast cancer in women with high genetic risk. Tumori 2006; 92: pp. 517-523.
20. Hagen A.I., Kvistad K.A., Maehle L., et. al.: Sensitivity of MRI versus conventional screening in the diagnosis of BRCA-associated breast cancer in a national prospective series. Breast 2007; 16: pp. 367-374.
21. Hoogerbrugge N., Kamm Y.J.L., Bult P., et. al.: The impact of a false-positive MRI on the choice for mastectomy in BRCA mutation carriers is limited. Ann Oncol 2008; 19: pp. 655-659.
22. Peters G., Anderson J., Longman G., et. al.: Magnetic resonance findings in women at high risk for developing breast cancer: an Australian feasibility study. J Med Imaging Radiat Oncol 2008; 52: pp. 29-35.
23. Reidl C.C., Ponhold L., Flory D., et. al.: Magnetic resonance imaging of the breast improves detection of invasive cancer, preinvasive cancer, and premalignant lesions during surveillance of women at high risk for breast cancer. Clin Cancer Res 2007; 13: pp. 6144-6152.
24. American College of Radiology: Breast Imaging Reporting and Data System (BI-RADS) Atlas.2003.American College of RadiologyReston, VA