
Rationale and Objectives
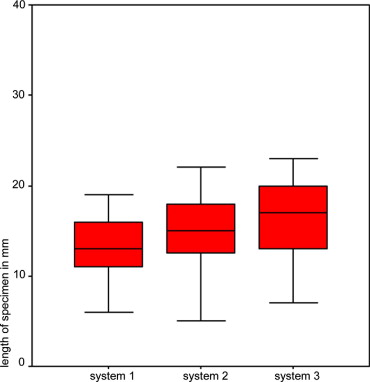
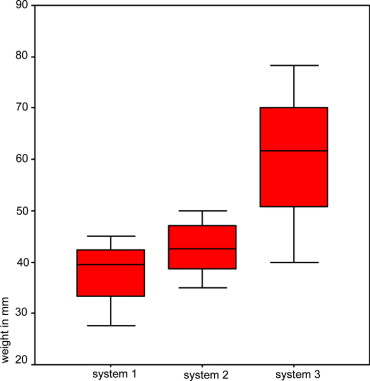
To compare three commercially available vacuum-assisted breast biopsy systems for tissue yield, length and fragmentation of specimens.
Materials and Methods
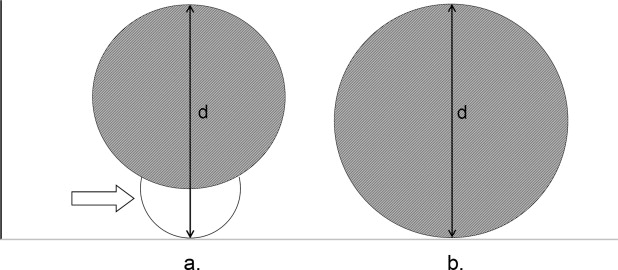
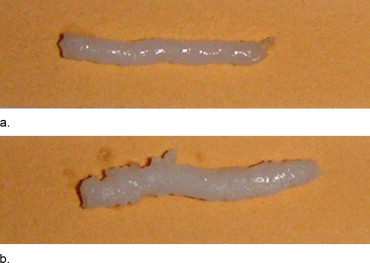
Specimens were acquired from radiolucent (bacon) and radioopaque (turkey breast) tissue using three different commercially available vacuum-assisted breast biopsy devices. Two systems (system 1 and 2) were equipped with 11 G needles, one system (system 3) with a 9 G needle. As for systems 1 and 2 a second chamber for applying the vacuum is attached to the needle, the external maximum diameter was identical for all three systems. 48 specimens were taken out for each tissue type and for each device. Specimens were measured for total weight, individual length, and number of fragments. Differences between groups were analyzed using analysis of variance (ANOVA) and Student’s t-test.
Results
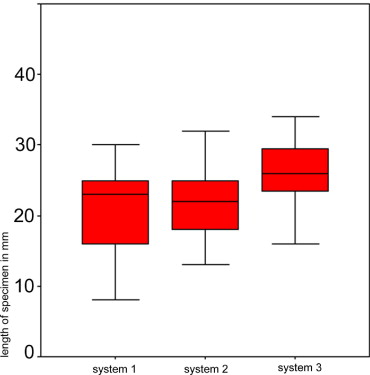
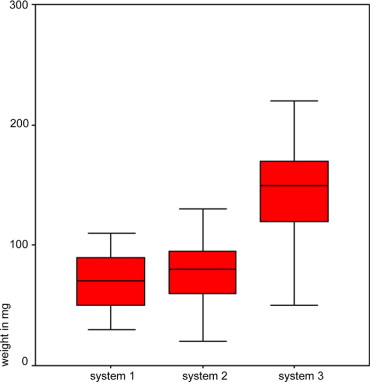
For both tissue types, system 1 and 2 showed similar results, for system 3 tissue weight and length of specimens were larger. Differences in lengths and weight were statistically significant between system 1 and 3 and system 2 and 3 (ANOVA, P < 0.05). Differences between length and weight were statistically significant between tissue 1 and 2 for all devices (t-Test < 0.05).
Conclusion
As for system 3 a larger tissue yield was obtained with the same number of specimens compared to systems 1 and 2, it can be assumed that the same diagnostic accuracy as for systems 1 and 2 may be achieved for system 3 with less passes through tissue.
Many breast lesions depicted by mammography or other imaging modalities have an uncharacteristic appearance. This is why there is a high demand for a reliable minimally invasive diagnostic tool with a high sensitivity and specificity. Various minimal invasive techniques for histologic diagnosis of focal breast lesions depicted by imaging modalities are available today, such as fine-needle aspiration cytology (FNAC), core-needle biopsy, and vacuum-assisted biopsy ( ). While in the past most breast biopsies were performed using FNAC, vacuum-assisted biopsy is increasingly used for confirmation of suspicious breast lesions ( ). This biopsy technique has been available at specialized centers since 1996 ( ). The most important advantage over other biopsy techniques is that larger tissue cores are obtained ( ), which reduces the rate of underestimation of breast lesions (e.g., diagnosis of atypical ductal hyperplasia on the basis of core biopsy versus invasive cancer based on open biopsy) and improves surgical planning ( ). Many publications recommend obtaining at least 12 specimens when vacuum-assisted breast biopsy is performed ( ). Most recommendations are based on 11-gauge biopsy, which is the most widely used technique. However, other vacuum-assisted biopsy devices with different probe systems have since become available. While older systems (Mammotome and Vacora) from Ethicon Endosurgery (Cincinnati, OH) and Bard (C.R. Bard, Murray Hill, NJ) that have been on the market for some time have been tested in various phantom studies ( ), the breast biopsy device from ATEC Suros (Suros Surgical Systems, Indianapolis, IN), to the best of our knowledge, has not been compared with conventional systems previously. Because the double-lumen needle of the Ethicon biopsy device increases the overall outer diameter, we compared the Ethicon device for obtaining an 11-gauge biopsy core with the 9-gauge ATEC Suros biopsy system, in order to compare two systems with identical overall outer diameters. The Bard system uses 10-gauge needles with an outer diameter that differs from that of the Ethicon and Suros biopsy systems; this is why we did not include the Bard system in our comparison. Moreover, the Bard breast biopsy unit is based on a different working principle (use of an insertion guide, withdrawal of the entire probe with each sampling step, vacuum not created externally as with the Ethicon and ATEC Suros systems).
The aim of the study presented here is to compare two Ethicon breast biopsy systems (Ethicon Mammotome Biopsys [system 1] and Ethicon Mammotome ST [system 2]) and a Suros Surgical Systems biopsy device (ATEC [system 3]) in terms of the amount of tissue that is obtained in a breast parenchyma phantom. As the diagnostic accuracy increases when more tissue is available for histology, the preferred system for vacuum-assisted biopsy would be the one with the highest tissue yield for a given number of specimens ( ). The only end point of this study is to determine differences between the three systems with regard to the average weight of biopsy specimens, core length, and degree of fragmentation.
Get Radiology Tree app to read full this article<
Materials and methods
Configuration of the Breast Biopsy Systems
Shared features
Get Radiology Tree app to read full this article<
Differences
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Tissue Sampling
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Geometry
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Time
Get Radiology Tree app to read full this article<
Disadvantages of the Systems
Ethicon Mammotome (system 1)
Get Radiology Tree app to read full this article<
Ethicon ST (system 2)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ATEC Suros (system 3)
Get Radiology Tree app to read full this article<
Statistical Analysis
Results in turkey breast
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results in bacon
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison between turkey breast and bacon for systems 1–3
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Heywang-Kobrunner S.H., Schaumloffel U., et. al.: Minimally invasive stereotaxic vacuum core breast biopsy. Eur Radiol 1998; 8: pp. 377-385.
2. Lomoschitz F.M., Helbich T.H., Rudas M., et. al.: Stereotactic 11-gauge vacuum-assisted breast biopsy: Influence of number of specimens on diagnostic accuracy. Radiology 2004; 232: pp. 897-903.
3. Helbich T.H., Matzek W., Fuchsjager M.H.: Stereotactic and ultrasound-guided breast biopsy. Eur Radiol 2004; 14: pp. 383-393.
4. Liberman L., Bracero N., Morris E., et. al.: MRI-guided 9-gauge vacuum-assisted breast biopsy: Initial clinical experience. AJR Am J Roentgenol 2005; 185: pp. 183-193.
5. Oyama T., Koibuchi Y., McKee G.: Core needle biopsy (CNB) as a diagnostic method for breast lesions: Comparison with fine needle aspiration cytology (FNA). Breast Cancer 2004; 11: pp. 339-342.
6. Otto R.: Interventional ultrasound. Eur Radiol 2002; 12: pp. 283-287.
7. Muller-Schimpfle M., Wersebe A., Xydeas T., et. al.: Microcalcifications of the breast: How does radiologic classification correlate with histology?. Acta Radiol 2005; 46: pp. 774-781.
8. Smith W.L., Surry K.J., Kumar A., et. al.: A Comparison of core needle breast biopsy techniques: Freehand versus three-dimensional US guidance. Acad Radiol 2002; 9: pp. 541-550.
9. Litherland J.: The role of needle biopsy in the diagnosis of breast lesions. Breast 2001; 10: pp. 383-387.
10. Fischmann A., Pietsch-Breitfeld B., Muller-Schimpfle M., et. al.: [Radiologic-histopathologic correlation of microcalcifications from 11g vacuum biopsy: analysis of 3196 core biopsies]. Rofo 2004; 176: pp. 538-543.
11. Meyer J.E., Smith D.N., DiPiro P.J., et. al.: Stereotactic breast biopsy of clustered microcalcifications with a directional, vacuum-assisted device. Radiology 1997; 204: pp. 575-576.
12. Jackman R.J., Marzoni F.A., Nowels K.W.: Percutaneous removal of benign mammographic lesions: Comparison of automated large-core and directional vacuum-assisted stereotactic biopsy techniques. AJR Am J Roentgenol 1998; 171: pp. 1325-1330.
13. Jackman R.J., Rodriguez-Soto J.: Breast microcalcifications: Retrieval failure at prone stereotactic core and vacuum breast biopsy—Frequency, causes, and outcome. Radiology 2006; 239: pp. 61-70.
14. Burbank F., Forcier N.: Tissue marking clip for stereotactic breast biopsy: Initial placement accuracy, long-term stability, and usefulness as a guide for wire localization. Radiology 1997; 205: pp. 407-415.
15. Philpotts L.E., Shaheen N.A., Carter D., et. al.: Comparison of rebiopsy rates after stereotactic core needle biopsy of the breast with 11-gauge vacuum suction probe versus 14-gauge needle and automatic gun. AJR Am J Roentgenol 1999; 172: pp. 683-687.
16. Fahrbach K., Sledge I., Cella C., et. al.: A comparison of the accuracy of two minimally invasive breast biopsy methods: A systematic literature review and meta-analysis. Arch Gynecol Obstet 2006; 274: pp. 63-73.
17. Brem R.F., Schoonjans J.M., Goodman S.N., et. al.: Nonpalpable breast cancer: Percutaneous diagnosis with 11- and 8-gauge stereotactic vacuum-assisted biopsy devices. Radiology 2001; 219: pp. 793-796.
18. Heywang-Kobrunner S.H.: New possibilities of diagnostic imaging and intervention. Curr Probl Cancer 2003; 27: pp. 32-38.
19. Lehman C.D., Aikawa T.: MR-guided vacuum-assisted breast biopsy: Accuracy of targeting and success in sampling in a phantom model. Radiology 2004; 232: pp. 911-914.
20. Sittek H., Linsmeier E., Perlet C., et. al.: [Preoperative marking and biopsy of nonpalpable breast lesions with a guidance system for the open Magnetom]. Radiologe 2000; 40: pp. 1098-1105.
21. Obenauer S., Grabbe E., Knollmann F.: [Value of MR-guided localization and biopsy in breast lesions]. Rofo 2006; 178: pp. 477-483.
22. Moche M., Schmitgen A., Schneider J.P., et. al.: [First clinical experience with extended planning and navigation in an interventional MRI unit]. Rofo 2004; 176: pp. 1013-1020.
23. Berg W.A., Krebs T.L., Campassi C., et. al.: Evaluation of 14- and 11-gauge directional, vacuum-assisted biopsy probes and 14-gauge biopsy guns in a breast parenchymal model. Radiology 1997; 205: pp. 203-208.
24. Heywang-Kobrunner S.H., Schreer I., Decker T., et. al.: Interdisciplinary consensus on the use and technique of vacuum-assisted stereotactic breast biopsy. Eur J Radiol 2003; 47: pp. 232-236.
25. Velanovich V., Lewis F.R., Nathanson S.D., et. al.: Comparison of mammographically guided breast biopsy techniques. Ann Surg 1999; 229: pp. 625-630. discussion 630–623