
Rationale and Objectives
The study aimed to prospectively evaluate the radiation dose reduction potential and image quality (IQ) of a high-concentration contrast media (HCCM) injection protocol in combination with a low tube current (mAs) in coronary computed tomography angiography.
Materials and Methods
Eighty-one consecutive patients (mean age: 62 years; 34 females; body mass index: 18–31) were included and randomized-assigned into two groups. All computed tomography (CT) examinations were performed in two groups with the same tube voltage (100 kV), flow rate of contrast medium (5.0 mL/s), and iodine dose (22.8 g). An automatic mAs and low concentration contrast medium (300 mgI/mL) were used in group A, whereas effective mAs was reduced by a factor 0.6 along with HCCM (400 mgI/mL) in group B. Radiation dose was assessed (CT dose index [CTDI vol ] and dose length product), and vessel-based objective IQ for various regions of interest (enhancement, noise, signal-to-noise ratio, and contrast-to-noise ratio), subjective IQ, noise, and motion artifacts were analyzed overall and vessel-based with a 5-point Likert scale.
Results
The CT attenuation of coronary arteries and image noise in group B were significantly higher than those in group A (ranges: 507.5–548.1 Hounsfield units vs 407.5–444.5 Hounsfield units; and 20.3 ± 8.6 vs 17.7 ± 8.0) ( P ≤ 0.0166). There was no significant difference between the two groups in signal-to-noise ratio, contrast-to-noise ratio, and subjective IQ of coronary arteries (29.4–31.7, 30.0–37.0, and medium score of 5 in group A vs 29.4–32.4, 27.7–36.3, and medium score of 5 in group B, respectively, P ≥ 0.1859). Both mean CTDI vol and dose length product in group B were 58% of those of group A.
Conclusions
HCCM combined with low tube current allows dose reduction in coronary computed tomography angiography and does not compromise IQ.
Introduction
Coronary artery disease (CAD) is one of the leading causes of morbidity and mortality worldwide. With the advancement in technology efforts to increase the accuracy in diagnosing CAD, coronary computed tomography angiography (CCTA) is an efficient and reliable modality for CAD diagnosis and is well established in routine clinical practice . Over the last decade, radiation concerns in radiology have been increased since the annual medical radiation dose per capita increased about sixfold to 3.0 mSv . CT represents only about 7% of all diagnostic imaging examinations using ionizing radiation, but it is responsible for more than 50% of the cumulative radiation exposure in Western countries . Currently, several technical improvements for radiation dose reduction in computed tomography (CT) have been developed. The use of a low kilovoltage (kV) is one of these options to reduce radiation dose in CCTA. Lower tube voltage causes a higher attenuation for iodinated contrast media (CM) and thus a higher enhancement in the coronary arteries is observed . At the same time, noise is considerably increased since low kV also reduces the total number of emitted X-ray photons, which needs to be compensated by a parallel increase of the effective mAs. A fundamental principle in radiation dose reduction protocols follows the approach to keep constant in the signal-to-noise ratio (SNR) . Because of the higher iodine signal achieved in low kV exams, a higher noise can be acceptable, which means that the compensatory increase in mAs needs to be moderate . An alternative or additional option, with same radiation dose reduction principle as low kV does, is to enhance the signal by increasing the iodine contrast. Likewise, this would allow for a (further) reduction of the reference mAs compared to an exam with a standard iodine contrast. CCTA is a typical “first pass” examination where the iodine delivery rate (IDR) becomes a crucial contrast injection parameter to determine enhancement . Using high-concentration contrast media (HCCM) is a possible approach to achieve high vessel signal in CT angiography by increasing the IDR, which may compensate for a reduced radiation dose and maintain the diagnostic image quality. Therefore, the combination of increased concentration of CM and reduced tube current-time product is an interesting concept to save radiation dose and to reserve image quality. This concept has been applied in CT angiography of the aorta and the pulmonary arteries , but not yet in CCTA. Specifically, sufficient overall image quality in CCTA is mandatory for adequately visualizing smaller vessels, so concerns may exist that big radiation dose reduction concepts might be limited.
The objective of this study was to test and assess whether radiation dose can be reduced with a “high contrast—low mAs” approach without compromising image quality in a vessel-based assessment. The hypothesis of this study was that a high IDR protocol using high concentration CM would enable us to lower the tube current time product and radiation exposure compared to a standard injection protocol while maintaining image quality.
Materials and Methods
Study Population
Get Radiology Tree app to read full this article<
Imaging and Injection Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Subjective Image Quality Assessment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Objective Image Quality Assessment
Get Radiology Tree app to read full this article<
Assessment of Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
TABLE 1
Patient Demographic Data and Dosimetric Parameters for Coronary CT Angiography Studies
Parameter Group A Group B_Z_ Value_F_ Value_P_ Value Patient age (y) 61.8 ± 11.5 62.4 ± 12.8 −0.435 — 0.6637 Sex (male/female) 12/29 13/27 — 0.813 0.4700 Height (cm) 164.1 ± 9.1 166.7 ± 6.9 −1.362 — 0.1731 Weight (kg) 67.0 ± 11.7 69.1 ± 10.3 −0.700 — 0.4840 BMI (kg/m2) 24.8 ± 3.2 24.8 ± 2.9 −0.208 — 0.8353 BSA (m2) 1.7 ± 0.2 1.8 ± 0.2 −0.825 — 0.4096 Heart rate (bpm) 64.0 ± 9.5 68.2 ± 11.5 −1.437 — 0.1508 Calcium score 2 (0–32) 0 (0–57) 1.014 — 0.3105 Contrast media injection CM concentration (mgI/mL) 300 400 — — — CM volume (mL) 76 57 — — — Iodine dose (g) 22.8 22.8 — — — CM flow rate (mL/s) 5.0 5.0 — — — Iodine delivery rate (grI/s) 1.5 2.0 — — — Coronary CT angiography — Tube voltage (kV) 100 100 — — — Effective tube current—time product per tube (mAs) 236.0 ± 52.8 157.3 ± 39.2 5.854 — <0.0001 Radiation dose CTDI vol (mGy) 23.5 ± 6.2 13.6 ± 3.9 6.499 — <0.0001 DLP (mGy •cm) 324.0 ± 86.2 187.5 ± 54.4 6.494 — <0.0001 Effective dose (mSv) 4.5 ± 1.2 2.6 ± 0.8 6.441 — <0.0001
BMI, body mass index; bpm, beats per minute; BSA, body surface area; CM, contrast media; CTDI, CT dose index; DLP, dose length product.
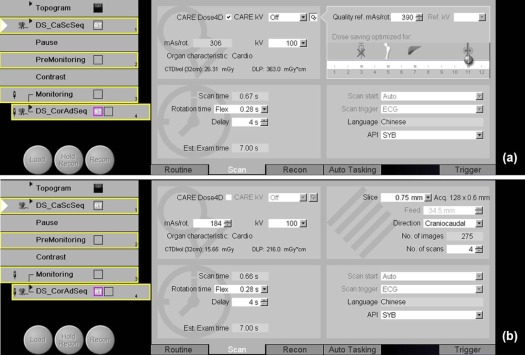
Notes: Patients in group A received a CM with an iodine concentration of 300 mgI/mL (Ultravist, Bayer HealthCare, Leverkusen, Germany) and automated tube current (Care Dose4D, Siemens Healthcare Sector). Patients in group B received a CM with an iodine concentration of 400 mgI/mL (Iomeron 400, Bracco Sine, Shanghai, China) and reduced tube current by factor 0.6 (changed the mAs value, which can be seen after the topogram). In line with the mAs reduction the mean CTDI vol and DLP were significantly lower with group B than with group A. Consequently, the mean effective dose was significantly lower with group B than with group A, a mean reduction of 42%.
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Subjective Image Quality Analysis
Get Radiology Tree app to read full this article<
TABLE 2
Subjective image assessment of different anatomic regions for the two groups
Parameter Group A Group B Pearson χ 2 P Value Image quality Overall 5 (5-5) 5 (5-5) 0.1877 0.6650 Left main coronary artery 5 (5-5) 5 (5-5) — >0.999 Left anterior descending artery 5 (5-5) 5 (5-5) — >0.999 Right coronary artery 5 (5-5) 5 (5-5) 0.0003 0.986 Circumflex artery 5 (5-5) 5 (5-5) 0.3210 0.571 Image noise Overall 5 (4-5) 4 (3-4) 30.3949 <0.0001 Left main coronary artery 5 (5-5) 4 (4-5) 31.4521 <0.0001 Left anterior descending artery 5 (5-5) 4 (4-5) 30.8617 <0.0001 Right coronary artery 5 (5-5) 4 (4-4) 29.6985 <0.0001 Circumflex artery 5 (5-5) 4 (4-5) 19.1256 <0.0001 Motion artifacts Overall 4 (4-4) 4 (4-4) 0.1877 0.6650 Left main coronary artery 4 (4-4) 4 (4-4) — >0.999 Left anterior descending artery 4 (4-4) 4 (4-4) 0.9878 0.320 Right coronary artery 4 (4-4) 4 (4-4) 0.9878 0.320 Circumflex artery 4 (4-4) 4 (4-4) 1.0378 0.308
CM, contrast media.
Notes: Patients in group A received a CM with an iodine concentration of 300 mgI/mL (Ultravist, Bayer HealthCare, Leverkusen, Germany) and automated tube current (Care Dose4D, Siemens Healthcare Sector). Patients in group B received a CM with an iodine concentration of 400 mgI/mL (Iomeron 400, Bracco Sine, Shanghai, China) and reduced tube current by factor 0.6 (changed the mAs value, which can be seen after the topogram). Subjective image quality analyses generally revealed excellent ratings with no statistically significant differences between two groups regarding overall image quality (group A: 5 [5-5 {25%–75% quartiles}] vs group B: 5 [5-5 {25%–75% quartiles}]; P = 0.6650) and motion artifacts (group A: 4 [4-4 {25%–75% quartiles}] vs. group B: 4 [4-4 {25%–75% quartiles}]; P = 0.6650). However, the overall image noise of group B was significantly higher than group A (group A: 5 [4-5 {25%–75% quartiles}] vs. group B: 4 [3-4 {25%–75% quartiles}]; P < 0.0001).
Get Radiology Tree app to read full this article<
Objective Image Quality Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Objective image assessment of different anatomic regions for the two groups
Parameter Group A Group B_Z_ Value_P_ Value Mean attenuation (HU) Pericardial fat tissue −112.8 ± 11.7 −114.6 ± 7.4 0.812 0.4166 Ascending aorta 410.9 ± 69.4 504.4 ± 91.1 −4.397 <0.0001 Left main coronary artery 419.8 ± 77.4 519.8 ± 97.5 −4.567 <0.0001 Left anterior descending artery 413.1 ± 69.7 512.4 ± 104.0 −4.411 <0.0001 Right coronary artery 444.5 ± 97.6 548.1 ± 104.4 −4.119 <0.0001 Circumflex artery 407.5 ± 84.8 507.5 ± 113.8 −4.086 <0.0001 Mean SNR Ascending aorta 29.4 ± 13.1 29.4 ± 15.3 0.236 0.8133 Left main coronary artery 30.2 ± 14.0 30.2 ± 15.4 0.128 0.8985 Left anterior descending artery 29.6 ± 13.5 30.4 ± 17.7 0.005 0.9962 Right coronary artery 31.7 ± 15.0 32.4 ± 17.5 0.184 0.8539 Circumflex artery 28.9 ± 12.7 29.9 ± 17.9 0.113 0.9097 Mean CNR Ascending aorta 17.5 ± 3.0 16.5 ± 2.6 1.323 0.1859 Left main coronary artery 30.9 ± 15.4 26.5 ± 9.7 0.883 0.3771 Left anterior descending artery 37.0 ± 22.3 36.3 ± 15.8 −0.128 0.8985 Right coronary artery 30.0 ± 14.7 27.7 ± 14.3 0.845 0.3978 Circumflex artery 31.0 ± 13.8 28.2 ± 13.7 1.294 0.1956
CM, contrast media; CNR, contrast-to-noise ratio; HU, Hounsfield unit; ROI, region of interest; SNR, signal-to-noise ratio.
Notes: Patients in group A received a CM with an iodine concentration of 300 mgI/mL (Ultravist, Bayer HealthCare, Leverkusen, Germany) and automated tube current (Care Dose4D, Siemens Healthcare Sector). Patients in group B received a CM with an iodine concentration of 400 mgI/mL (Iomeron 400, Bracco Sine, Shanghai, China) and reduced tube current by factor 0.6 (changed the mAs value, which can be seen after the topogram). Mean attenuation values were significantly higher with group B than with group A in all arterial ROIs ( P < 0.0001). Quantitative image noise was significantly higher with group B (20.0 ± 7.0) than group A (16.1 ± 5.3) ( P = 0.0166). For SNR and CNR, no significantly difference was found between group A and group B for all arterial ROIs ( P ≥ 0.1859). This validates the assumptions that were made above to estimate the mAs reduction factor 0.6 (was based on the assumption of keeping SNR constant).
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Layritz C., Schmid J., Achenbach S., et. al.: Accuracy of prospectively ECG-triggered very low-dose coronary dual-source CT angiography using iterative reconstruction for the detection of coronary artery stenosis: comparison with invasive catheterization. Eur Heart J Cardiovasc Imaging 2014; 15: pp. 1238-1245.
2. Rief M., Kranz A., Hartmann L., et. al.: Computer-aided CT coronary artery stenosis detection: comparison with human reading and quantitative coronary angiography. Int J Cardiovasc Imaging 2014; 30: pp. 1621-1627.
3. Nakazato R., Otake H., Konishi A., et. al.: Atherosclerotic plaque characterization by CT angiography for identification of high-risk coronary artery lesions: a comparison to optical coherence tomography. Eur Heart J Cardiovasc Imaging 2015; 16: pp. 373-379.
4. Sun K., Li K., Han R., et. al.: Evaluation of high-pitch dual-source CT angiography for evaluation of coronary and carotid-cerebrovascular arteries. Eur J Radiol 2015; 84: pp. 398-406.
5. Madhok R., Aggarwal A.: Comparison of 128-slice dual source CT coronary angiography with invasive coronary angiography. J Clin Diagn Res 2014; 8: pp. C8-C11.
6. Ropers D., Pohle F.K., Kuettner A., et. al.: Diagnostic accuracy of noninvasive coronary angiography in patients after bypass surgery using 64-slice spiral computed tomography with 330-ms gantry rotation. Circulation 2006; 114: pp. 2334-2341. 2334
7. Einstein A.J.: Effects of radiation exposure from cardiac imaging: how good are the data?. J Am Coll Cardiol 2012; 59: pp. 553-565.
8. Heusch P., Lanzman R.S., Aissa J., et. al.: Evaluation of a high iodine delivery rate in combination with low tube current for dose reduction in pulmonary computed tomography angiography. J Thorac Imaging 2014; 5: pp. 293-297.
9. Meyer M., Haubenreisser H., Schoepf U.J., et. al.: Closing in on the K edge: coronary CT angiography at 100, 80, and 70 kV-initial comparison of a second- versus a third-generation dual-source CT system. Radiology 2014; 273: pp. 373-382.
10. Tack D., Kalra M.K., Gevenois P.A.: Radiation dose from multidetector CT.2012.SpringerBerlin Heidelberg
11. Heiland S., Erb G., Ziegler S., et. al.: Where contrast agent concentration really matters—a comparison of CT and MRI. Invest Radiol 2010; 45: pp. 529-537.
12. Bae K.T.: Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology 2010; 256: pp. 32-61.
13. Iezzi R., Cotroneo A.R., Giammarino A., et. al.: Low-dose multidetector-row CT-angiography of abdominal aortic aneurysm after endovascular repair. Eur J Radiol 2011; 79: pp. 21-28.
14. Schwarz F., Grandl K., Arnoldi A., et. al.: Lowering radiation exposure in CT angiography using automated tube potential selection and optimized iodine delivery rate. AJR Am J Roentgenol 2013; 200: pp. W628-W634.
15. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
16. European Commission : European guidelines on quality criteria for computed tomography.1998.European CommissionLuxembourg
17. The 2007 recommendations of the international commission on radiological protection. ICRP publication 103. Ann ICRP 2007; 37: pp. 1-332.
18. Leschka S., Stolzmann P., Schmid F.T., et. al.: Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol 2008; 18: pp. 1809-1817.
19. Schindera S.T., Nelson R.C., Yoshizumi T., et. al.: Effect of automatic tube current modulation on radiation dose and image quality for low tube voltage multidetector row CT angiography: phantom study. Acad Radiol 2009; 16: pp. 997-1002.
20. Cademartiri F., de Monye C., Pugliese F., et. al.: High iodine concentration contrast material for noninvasive multislice computed tomography coronary angiography: iopromide 370 versus iomeprol 400. Invest Radiol 2006; 41: pp. 349-353.
21. Behrendt F.F., Plumhans C., Keil S., et. al.: Contrast enhancement in chest multidetector computed tomography: intraindividual comparison of 300 mg/ml versus 400 mg/ml iodinated contrast medium. Acad Radiol 2009; 16: pp. 144-149.
22. Muhlenbruch G., Behrendt F.F., Eddahabi M.A., et. al.: Which iodine concentration in chest CT?—a prospective study in 300 patients. Eur Radiol 2008; 18: pp. 2826-2832.
23. MacKenzie J.D., Nazario-Larrieu J., Cai T., et. al.: Reduced-dose CT: effect on reader evaluation in detection of pulmonary embolism. AJR Am J Roentgenol 2007; 189: pp. 1371-1379.
24. Hansmann J., Fink C., Jost G., et. al.: Impact of iodine delivery rate with varying flow rates on image quality in dual-energy CT of patients with suspected pulmonary embolism. Acad Radiol 2013; 20: pp. 962-971.
25. Schimmoller L., Lanzman R.S., Heusch P., et. al.: Impact of organ-specific dose reduction on the image quality of head and neck CT angiography. Eur Radiol 2013; 23: pp. 1503-1509.
26. Szucs-Farkas Z., Kurmann L., Strautz T., et. al.: Patient exposure and image quality of low-dose pulmonary computed tomography angiography: comparison of 100- and 80-kVp protocols. Invest Radiol 2008; 43: pp. 871-876.
27. Uehara M., Takaoka H., Kobayashi Y., et. al.: Diagnostic accuracy of 320-slice computed-tomography for detection of significant coronary artery stenosis in patients with various heart rates and heart rhythms compared with conventional coronary-angiography. Int J Cardiol 2013; 167: pp. 809-815.
28. Iyengar S.S., Morgan-Hughes G., Ukoumunne O., et. al.: Diagnostic accuracy of high-definition CT coronary angiography in high-risk patients. Clin Radiol 2016; 71: pp. 151-158.
29. Andreini D., Pontone G., Mushtaq S., et. al.: Coronary stent evaluation with coronary computed tomographic angiography: comparison between low-osmolar, high-iodine concentration iomeprol-400 and iso-osmolar, lower-iodine concentration iodixanol-320. J Cardiovasc Comput Tomogr 2014; 8: pp. 44-51.
30. Maffei E., Martini C., Arcadi T., et. al.: Plaque imaging with CT coronary angiography: effect of intra-vascular attenuation on plaque type classification. World J Radiol 2012; 4: pp. 265-272.