
Rationale and Objectives
We sought to assess the performance of a real-time interactive pulmonary nodule analysis system for evaluation of chest digital radiographic (DR) images in a routine clinical environment.
Materials and Methods
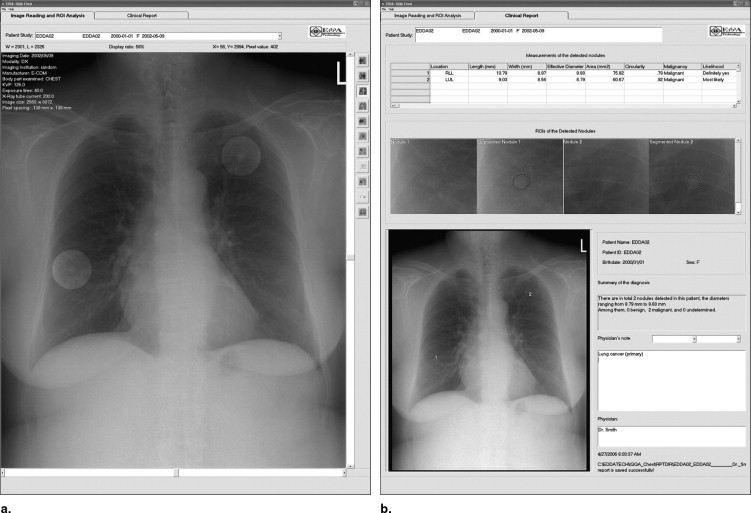
A real-time interactive pulmonary nodule analysis system for chest DR image softcopy reading (IQQA-Chest; EDDA Technology, Princeton Junction, NJ) was used in daily practice with a Picture Archiving and Communication System in a National Cancer Institute−designated cancer teaching hospital. Patients referred for follow-up of known cancer underwent digital chest radiography. Posteroanterior and lateral DR images were first read by resident radiologists along with experienced chest radiologists using a Picture Archiving and Communication System work station. The computer-assisted detection (CAD) program was subsequently applied to the posteroanterior DR images, and changes (if any) in diagnosis were recorded. For reference standard, a follow-up chest radiograph at least 6 months following the initial examination or a follow-up computed tomographic scan of the chest within 3 months was used to establish diagnostic accuracy.
Results
Of 324 DR examinations, follow-up imaging according to our parameters was available for 214 patients (67%). Lung nodules were found and subsequently confirmed in 35 patients (10%) without CAD. Using CAD, nodules were found and subsequently confirmed in 51 patients (15%), improving sensitivity from 63.8% (95% confidence interval [CI], 0.49%−0.76%) to 92.7% (95% CI, 0.82%−0.98%) ( P < .0001, McNemar). Nodules were subsequently proved to be malignant in five of the 16 additional cases (31%). False-positive readings increased from three to six cases; specificity decreased from 98.1% (95% CI, 0.95%−0.99%) to 96.2% (95% CI, 0.92%−0.98%) (not significant). There were 153 true-negative cases (71.4%).
Conclusions
This study suggests that the interpretation of chest radiographs for lung nodules can be improved using an automated CAD nodule detection system. This improvement in reader performance comes with a minimal number of false-positive interpretations.
Chest radiography remains a popular modality for the surveillance of pulmonary metastatic disease in patients with known malignancies. It is vitally important to detect pulmonary nodules as early as possible in this patient population in an effort to initiate timely treatment. It is well known, however, that chest radiography is not very sensitive for demonstrating small nodules, especially those less than 1 cm in diameter ( ). Furthermore, perception studies repeatedly have shown that the detection rate of pulmonary nodules on chest films is poor, with radiologist performances ranging from 50% to 70% ( ). It has been argued that computed tomography (CT) is not suitable for the screening of lung cancer ( ), and likewise, the greater expense and substantially greater radiation exposures preclude CT from serving as a surveillance examination for metastatic disease in the vast majority of patients.(
Computer-assisted detection (CAD) software has been developed for a range of applications, including mammography, and chest CT ( ). In an effort to obviate low nodule detection rates inherent with chest radiography, the application of CAD to film interpretation may result in a significant improvement in overall reader performance ( ). Several studies have already shown that incorporating CAD into routine chest film interpretation has improved reader performance significantly ( ). Two previous studies reported that lung nodule detection rates improved when applied to both lung cancer screening ( ) and cancer follow-up radiographs ( ). The aim of this project was to investigate the benefit of CAD for nodule detection on chest films obtained in daily practice on patients under surveillance for metastatic disease.(
Materials and methods
Patient Selection
Get Radiology Tree app to read full this article<
Chest Radiography
Get Radiology Tree app to read full this article<
Software Detection System
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Reading Protocol
Get Radiology Tree app to read full this article<
Reference Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Histological Cancer Types Referred for Follow-up Chest Radiographs (in Order of Frequency)
Cancer Type No. ( N = 214) Renal cell cancer 24 Breast cancer 23 Lymphoma 21 Bladder cancer 19 Endometrial cancer 17 Testicular cancer 16 Ovarian cancer 16 Cervical cancer 15 Head/neck cancer 14 Colorectal cancer 12 Melanoma/skin cancer 10 Esophageal cancer 8 Hepatocellular cancer 7 Sarcoma 7 Pancreatic cancer 3 Prostate cancer 3 Stomach/duodenal cancer 3 Carcinosarcoma uterus 1 Brain tumor 1 Adrenal cancer 1 Adenocarcinoma (unknown primary) 1 Double tumors Ovarian/melanoma 1 Colon/breast 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Performance of Double-Read Chest Radiographs Without Additional Computer-Assisted Detection Software Being Used
Nodule Proven, n Nodule Absent, n Radiologist detected 35 3 Radiologist normal 20 156
Sensitivity: 35/55 (63.6%)
Specificity: 156/159 (98.1%)
Positive predictive value: 35/38 (92.1%)
Negative predictive value: 156/176 (88.6%)
Accuracy: 191/214 (89.2%)
Table 3
Performance of Double-Read Chest Radiographs With Additional Computer-Assisted Software Being Used
Nodule Proven, n Nodule Absent, n Radiologist + CAD detected 51 6 Radiologist + CAD normal 4 153
Sensitivity: 51/55 (92.7%)
Specificity: 153/159 (96.2%)
Positive predictive value: 51/57 (89.5%)
Negative predictive value: 153/157 (97.5%)
Accuracy: 204/214 (95.3%)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Samei E., Flynn M.J., Peterson E., Eyler W.R.: Subtle lung nodules: Influence of local anatomic variations on detection. Radiology 2003; 228: pp. 76-84.
2. Quekel L.G., Kessels A.G., Goei R., van Engelshoven J.M.: Miss rate of lung cancer on the chest radiograph in clinical practice. Chest 1999; 115: pp. 720-724.
3. Shah P.K., Austin J.H., White C.S., et. al.: Missed non–small cell lung cancer: Radiographic findings of potentially resectable lesions evident only in retrospect. Radiology 2003; 226: pp. 235-241.
4. Swensen S.J., Jett J.R., Sloan J.A., et. al.: Screening for lung cancer with low dose spiral computed tomography. Am J Respir Crit Care Med 2002; 165: pp. 508-513.
5. Doi K.: Current status and future potential of computer-aided diagnosis in medical imaging. Br J Radiol 2005; 78: pp. S3-S19.
6. Li F., Arimura H., Suzuk K., et. al.: Computer-aided detection of peripheral lung cancers missed at CT: ROC analyses without and with localization. Radiology 2005; 237: pp. 684-690.
7. Abe H., MacMahon H., Engelmann R., et. al.: Computer-aided diagnosis in chest radiography: Results of large-scale observer tests at the 1996–2001 RSNA scientific assemblies. Radiographics 2003; 23: pp. 255-265.
8. Das M., Muehlenbruch G., Mahnken A.H., et. al.: Small pulmonary nodules: Effect of two computer-aided detection systems on radiologist performance. Radiology 2006; 241: pp. 564-571.
9. MacMahon H., Engelmann R., Behlen F., et. al.: Computer aided diagnosis of pulmonary nodules: Results of a large scale observer test. Radiology 1999; 213: pp. 723-726.
10. Kakeda S., Moriya J., Sato H., et. al.: Improved detection of lung nodules on chest radiographs using a commercial computer-aided diagnosis system. AJR Am J Roentgenol 2004; 182: pp. 505-510.
11. Kobayashi T., Xu X.W., MacMahon H., Metz C.E., Doi K.: Effect of a computer-aided diagnosis scheme on radiologists’ performance in detection of lung nodules on radiographs. Radiology 1996; 199: pp. 843-848.
12. Song W., Fan L., Xie Y., Qian J.Z., Jin Z.: A study of inter-observer variations of pulmonary nodule marking and characterizing on DR images. Proc SPIE Med Imaging 2005; 5749: pp. 272-280.
13. Van Beek E., Mullan B., Stanford W., Thompson B.: Evaluation of a real-time interactive pulmonary nodule analysis system on chest digital radiographic images: A prospective study.Proceedings of the RSNA 92nd Scientific Assembly and Annual Meeting.2006.RSNAChicago, IL:pp. 570.
14. Wu N., Gamsu G., Czum J., et. al.: Detection of small pulmonary nodules using direct digital radiography and picture archiving and communication systems. J Thorac Imaging 2006; 21: pp. 27-31.