
Rationale and Objectives
To evaluate the role of apparent diffusion coefficient (ADC) in distinguishing ductal carcinoma in situ (DCIS) grades and identifying microinvasive and/or invasive disease in the preoperative evaluation of patients with core biopsy-proven DCIS.
Materials and Methods
Research Ethics Board-approved study with informed consent from 81 women (age, 36–84 years) scheduled for core-biopsy with results of 82 noninvasive breast carcinomas. All patients were assessed preoperatively by diffusion sequence in addition to contrast magnetic resonance imaging (MRI). Lesion morphology and ADC values were recorded. The Kruskal–Wallis or one-way analysis of variance test and Pearson correlation coefficient were used to study the association between ADC and MRI lesion characteristics. Logistic regression analysis was used to evaluate the ability of ADC to predict the presence of invasion.
Results
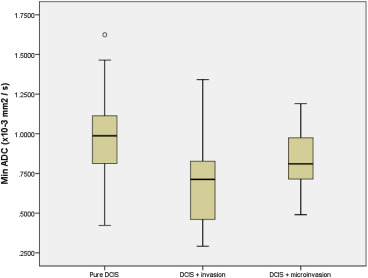
Surgical pathology demonstrated associated invasive cancer in 26.8%, microinvasion in 14.6%, and pure DCIS in 58.5%. The minimum regions of interest (ROI)–based ADC was significantly different among the following three groups ( P < .001, Kruskal–Wallis test): 0.98 × 10 −3 mm 2 /s ± 0.25 for pure DCIS, 0.82 × 10 −3 mm 2 /s ± 0.20 for DCIS with microinvasion, and 0.71 × 10 −3 mm 2 /s ± 0.27 for DCIS with invasive disease. Based on logistic regression analysis, the minimum ROI-based ADC of 0.56 × 10 −3 mm 2 /s was a significant predictor for invasive disease (odds ratio = 0.02, 95% confidence interval [0.002, 0.207], P = .001). Regardless of the field strength (1.5 vs. 3.0 T) ADC values of high-grade and non–high-grade DCIS were not significantly different.
Conclusions
Pure DCIS had the highest “ROI-based” ADC measured using 1.5 T or 3.0 T. The ADC was able to identify microinvasion or invasive cancer in biopsy-proven DCIS lesions but not to distinguish the DCIS grades.
Ductal carcinoma in situ (DCIS) of the breast is a preinvasive neoplasm characterized by a proliferation of malignant ductal epithelial cells that are confined within the basement membrane of preexisting duct and/or lobular units of the breast . Since the early 1980s, the prevalence of DCIS has been rising as a result of the adoption of widespread mammographic screening for breast cancer and the advances in mammographic techniques, image processing, and interpretation of digital imaging .
Magnetic resonance imaging (MRI) has been useful in the preoperative setting of invasive breast cancer . Specifically, dynamic contrast-enhanced (DCE) MRI has shown strong capability in the detection of invasive breast cancer with a sensitivity approaching 100% . The reported sensitivity of DCIS detection on MRI ranges from 77% to 96%, being largely impeded by challenges in distinguishing images suggestive of in situ cancer from benign and atypical proliferative processes, thus resulting in a higher false positive rate .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Design and Patient Selection
Get Radiology Tree app to read full this article<
MRI Examinations
Get Radiology Tree app to read full this article<
Imaging Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histologic Classification
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Comparison of Three Nuclear Grades of DCIS Stratified by the Presence or Absence of Microinvasion and/or Invasive Cancer in the Surgical Specimens
Microinvasion/Invasive Tumor DCIS Grades by Surgical Pathology Grade 1 DCIS Grade 2 DCIS Grade 3 DCIS All Grades Absent “pure DCIS,” n (%) 5 (71.4) 21 (70.0) 22 (48.9) 48 (58.5) DCIS + invasion, n (%) 2 (28.6) 7 (23.3) 13 (28.9) 22 (26.8) DCIS + micro invasion, n (%) 0 (0.0) 2 (6.7) 10 (22.2) 12 (14.6) Total 7 (100) 30 (100) 45 (100) 82 (100)
DCIS, ductal carcinoma in situ.
Note: Grades 1 and 2 DCIS are grouped into “non–high grade,” whereas grade 3 is “high grade.”
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Esserman L.J., Kumar A.S., Herrera A.F., et. al.: Magnetic resonance imaging captures the biology of ductal carcinoma in situ. J Clin Oncol 2006; 24: pp. 4603-4610.
2. Shiraishi A., Kurosaki Y., Maehara T., et. al.: Extension of ductal carcinoma in situ: histopathological association with MR imaging and mammography. Magn Reson Med Sci 2003; 2: pp. 159-163.
3. Iima M., Le Bihan D., Okumura R., et. al.: Apparent diffusion coefficient as an MR imaging biomarker of low-risk ductal carcinoma in situ: a pilot study. Radiology 2011; 260: pp. 364-372.
4. Rahbar H., Partridge S.C., Demartini W.B., et. al.: In vivo assessment of ductal carcinoma in situ grade: a model incorporating dynamic contrast-enhanced and diffusion-weighted breast MR imaging parameters. Radiology 2012; 263: pp. 374-382.
5. Neubauer H., Li M., Kuehne-Heid R., et. al.: High-grade and non high-grade ductal carcinoma in situ on dynamic MR mammography: characteristic findings for signal increase and morphological pattern of enhancement. Br J Radiol 2003; 76: pp. 3-12.
6. Jansen S.A., Newstead G.M., Abe H., et. al.: Pure ductal carcinoma in situ: kinetic and morphologic MR characteristics compared with mammographic appearance and nuclear grade. Radiology 2007; 245: pp. 684-691.
7. Kuhl C.: The current status of breast MR imaging. II. Current status of breast MR imaging. Radiology 2007; 244: pp. 672-691.
8. Raza S., Vallejo M., Chikarmane S.A., et. al.: Pure ductal carcinoma in situ: a range of MRI features. AJR 2008; 191: pp. 689-699.
9. Partridge S.C., Demartini W.B., Kurland B.F., et. al.: Quantitative diffusion-weighted MRI as an adjunct to conventional breast MRI for improved positive predictive value. AJR 2009; 193: pp. 1716-1722.
10. Charles-Edwards E.M., DeSouza N.M.: Diffusion-weighted magnetic resonance imaging and its application to cancer. Cancer Imaging 2006; 6: pp. 135-143.
11. Park M.J., Cha E.S., Kang B.J., et. al.: The role of diffusion-weighted imaging and the apparent diffusion coefficient (ADC) values for breast tumors. Korean J Radiol 2007; 8: pp. 390-396.
12. Thomassin-Naggara I., De Bazelaire C., Chopier J., et. al.: Diffusion-weighted MR imaging of the breast: advantages and pitfalls. Eur J Radiol 2013; 82: pp. 435-443.
13. Hirano M., Satake H., Ishigaki S., et. al.: Diffusion-weighted imaging of breast masses: comparison of diagnostic performance using various apparent diffusion coefficient parameters. AJR Am J Roentgenol 2012; 198: pp. 717-722.
14. Bogner W., Gruber S., Pinker K., et. al.: Diffusion-weighted MR for differentiation of breast lesions at 3.0 T: how does selection of diffusion protocols affect diagnosis?. Radiology 2009; 253: pp. 341-351.
15. Woodhams R., Matsunaga K., Iwabuchi K., et. al.: Diffusion-weighted imaging of malignant breast tumors: the usefulness of apparent diffusion coefficient (ADC) value and ADC map for the detection of malignant breast tumors and evaluation of cancer extension. J Comput Assist Tomogr 2005; 29: pp. 644-649.
16. Imamura T., Isomoto I., Sueyoshi E., et. al.: Diagnostic performance of ADC for non-mass-like breast lesions on MR imaging. Magn Reson Med Sci 2010; 9: pp. 217-225.
17. Scaranelo A.M., Eiada R., Jacks L.M., et. al.: Accuracy of unenhanced MR imaging in the detection of axillary lymph node metastasis: study of reproducibility and reliability. Radiology 2012; 262: pp. 425-434.
18. Cheng L., Bai Y., Zhang J., et. al.: Optimization of apparent diffusion coefficient measured by diffusion-weighted MRI for diagnosis of breast lesions presenting as mass and non-mass-like enhancement. Tumor Biol 2013; 34: pp. 1537-1545.
19. Partridge S.C., Mullins C.D., Kurland B.F., et. al.: Apparent diffusion coefficient values for discriminating benign and malignant breast MRI lesions: effects of lesion type and size. AJR Am J Roentgenol 2010; 194: pp. 1664-1673.
20. Morris E.A., Comstock C.E., Lee C.H., et. al.: ACR BI-RADS ® Magnetic Resonance Imaging..2013.American College of RadiologyReston, VA:
21. Lester S.C., Bose S., Chen Y.Y., et. al., Members of the Cancer Committee, College of American Pathologists: Protocol for the examination of specimens from patients with ductal carcinoma in situ of the breast. Arch Pathol Lab Med 2009; 133: pp. 15-25.
22. Rosen E.L., Smith-Foley S.A., DeMartini W.B., et. al.: BI-RADS MRI enhancement characteristics of ductal carcinoma in situ. Breast J 2007; 13: pp. 545-550.
23. Koh D.M., Collins D.J.: Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol 2007; 188: pp. 1622-1635.
24. Matsuoka A., Minato M., Harada M., et. al.: Comparison of 3.0-and 1.5-tesla diffusion-weighted imaging in the visibility of breast cancer. Radiat Med 2008; 26: pp. 15-20.
25. Kosior R.K., Wright C.J., Kosior J.C., et. al.: 3-Tesla versus 1.5-Tesla magnetic resonance diffusion and perfusion imaging in hyperacute ischemic stroke. Cerebrovasc Dis 2007; 24: pp. 361-368.
26. Saremi F., Jalili M., Sefidbakht S., et. al.: Diffusion-weighted imaging of the abdomen at 3 T: image quality comparison with 1.5-T magnet using 3 different imaging sequences. J Comput Assist Tomogr 2011; 35: pp. 317-325.
27. El Khouli R.H., Jacobs M.A., Mezban S.D., et. al.: Diffusion-weighted imaging improves the diagnostic accuracy of conventional 3.0-T breast MR imaging. Radiology 2010; 256: pp. 64-73.