
Rationale and Objectives
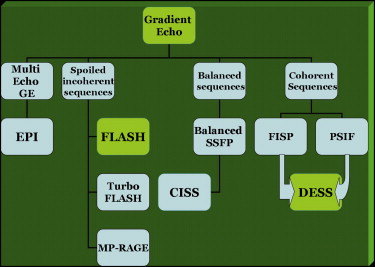
Accurate assessment of the morphology of sacroiliac joint (SIJ) bone cortex and cartilage bears importance in terms of detecting sacroiliitis in its earliest period. The aim of this study was to evaluate the efficacies of fat-saturated T1-weighted (T1WFS) spin-echo, three-dimensional (3D)-fast low angle shot (3D-FLASH), and 3D-double excitation in the steady-state (3D-DESS) sequences for the detection of SIJ cartilage and bone cortex abnormalities in patients with clinically suspected active sacroiliitis.
Materials and Methods
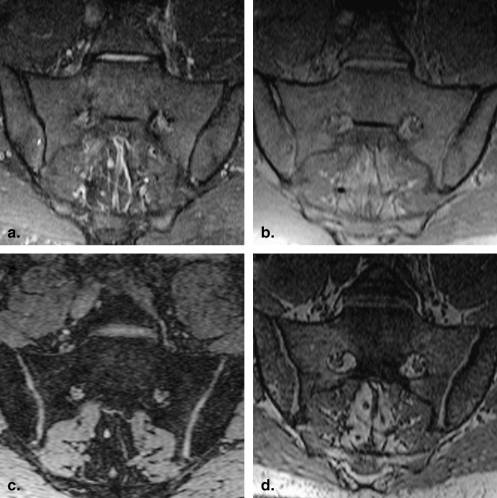
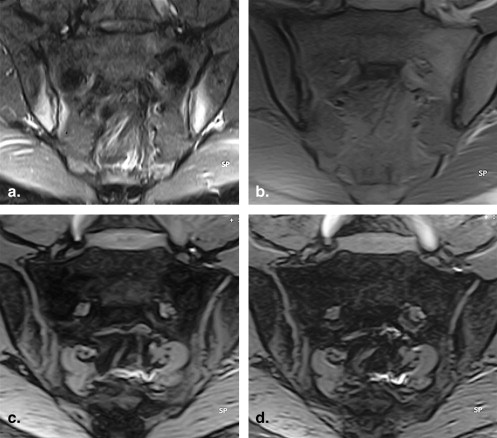
Magnetic resonance imaging (MRI) was performed in 9 controls and 30 patients with suspected active sacroiliitis. T1WFS, short tau inversion recovery, 3D-DESS with FS, 3D-FLASH with FS, postcontrast (the same precontrast T1WFS sequence) T1WFS, and subtracted images were obtained in all the cases. The bone cortex and cartilaginous morphology were visually scored on the T1WFS, 3D-DESS, and 3D-FLASH images. MRI findings were statistically evaluated.
Results
Active sacroiliitis was observed in 28 patients (49 SIJs) that were examined by postcontrast and subtracted images. T1WFS, 3D-DESS, and 3D-FLASH images revealed cartilage erosions in 26 (47 SIJs), 28 (55 SIJs), and 28 (55 SIJs) patients, respectively. Cartilage and bone cortex erosion scores in SIJs were significantly higher in 3D-DESS and 3D-FLASH images than in T1WFS images ( P < .05). Bone erosion scores assessed on T1WFS and 3D-FLASH images of active sacroiliitis patients, were found to be significantly different ( P < .05). A similar relationship was not determined between 3D-DESS and T1WFS sequences ( P > .05).
Conclusion
3D-FLASH sequence with FS is recognized as the most useful sequence for the detection of cartilaginous and cortical bone abnormalities.
The clinical diagnosis of sacroiliitis in patients with suspected spondyloarthropathy is difficult in the presence of radiographically normal sacroiliac joints or suspected findings . Early diagnosis of sacroiliitis is essential for therapeutic decision-making . Magnetic resonance imaging (MRI) has been reported to be better than plain radiographs and CT for investigation of active sacroiliitis . Furthermore, MRI is not, as computed tomography (CT), associated with radiation exposure. In the sacroiliac joint (SIJ), determination of hyperintense areas on short tau inversion recovery (STIR) images and observation of contrast-material enhancement on T1-weighted (W) images; both support active sacroiliitis . The earliest symptom of sacroiliitis is reported to be the contour irregularity and erosions on the cartilage surface . Accurate assessment of the morphology of joint cartilage–bone cortex bears importance in terms of detecting sacroiliitis in the earliest period.
Magnetic resonance (MR) sequences for cartilage visualization have been investigated by numerous studies, and the most useful MR sequence for SIJ cartilage imaging remains a question yet to be settled . Because three-dimensional (3D) double excitation in the steady-state (3D-DESS) sequence is cartilage-specific, it is known to have an excellent sensitivity in diagnosis of cartilage abnormities. Moreover, it is used in assessment of many other joint cartilages (eg, femorotibial joint cartilage), as well .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients and Controls
Get Radiology Tree app to read full this article<
Inclusion and Exclusion Criteria
Get Radiology Tree app to read full this article<
MR Examinations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Grading of Cortical Bone Erosions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Grading of Cartilage Morphology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Laboratory Tests
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Contrast-enhanced MRI Findings of Patient Group
Negative Unilateral Positive Bilateral Positive Total Sclerosis 2 1 27 30 Bone edema 2 3 25 30 SIJ-CE on T1WFS images 6 7 17 30 SIJ-CE on subtracted images 2 7 21 30
MRI, magnetic resonance imaging; SIJ, sacroiliac joint; CE, cartilage erosion; TI WFS, fat-saturated T1-weighted.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Cortical Bone and Cartilage Erosion Scores of Patient Group
Cartilage Erosions Cortical Bone Erosions Score of erosions T1WFS SIJs 3D-DESS SIJs 3D-FLASH SIJs T1WFS SIJs 3D-DESS SIJs 3D-FLASH SIJs Score 0 13 5 5 13 7 7 Score 1 32 11 13 38 18 20 Score 2 14 22 25 8 24 23 Score 3 1 22 17 1 11 10 Total 60 60 60 60 60 60
SIJs, sacroiliac joints; TI WFS, fat-saturated T1-weighted; 3D, three-dimensional; DESS, double excitation in the steady-state; FLASH, fast low angle shot.
Table 3
Spearman Correlation Analyses of Patients’ Cortical Bone Erosion Scores
T1WFS 3D-DESS 3D-FLASH Correlation coefficient 0.563 0.680P value < .001 < .001
TI WFS, fat-saturated T1-weighted; 3D, three-dimensional; DESS, double excitation in the steady-state; FLASH, fast low angle shot.
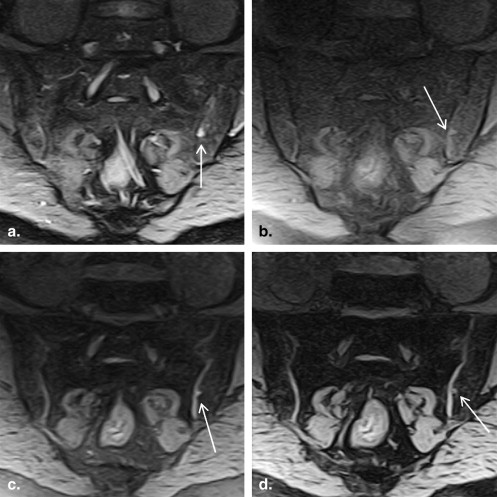
Table 4
Mean Cortical Bone Erosion Scores of Patient Group
Active Sacroiliitis T1WFS (Mean ± SD) 3D-DESS (Mean ± SD) 3D-FLASH (Mean ± SD) − 0.14 ± 0.1 1 ± 0.38 0.86 ± 0.26 + 1 ± 0.08 1.74 ± 0.12 1.6 ± 0.12P value .001 ∗ .98 .046 ∗
TI WFS, fat-saturated T1-weighted; 3D, three-dimensional; DESS, double excitation in the steady-state; FLASH, fast low angle shot; SD: standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Spearman Correlation Analyses of Patients’ Cartilaginous Erosion Scores
T1WFS 3D-DESS 3D-FLASH Correlation coefficient 0.569 0.699P value <.001 <.001
TI WFS, fat-saturated T1-weighted; 3D, three-dimensional; DESS, double excitation in the steady-state; FLASH, fast low angle shot;
Table 6
Mean Cartilaginous Erosion Scores of Patient Group
Active Sacroiliitis T1WFS (Mean ± SD) 3D-DESS (Mean ± SD) 3D-FLASH (Mean ± SD) − 0.43 ± 0.2 1.14 ± 0.46 0.86 ± 0.34 + 1.13 ± 0.1 2.13 ± 0.12 1.94 ± 0.12P value .023 ∗ .038 ∗ .009 ∗
TI WFS, fat-saturated T1-weighted; 3D, three-dimensional; DESS, double excitation in the steady-state; FLASH, fast low angle shot; SD: standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bollow M., Braun J., Hamm B., et. al.: Early sacroiliitis in patients with spondyloarthropathy: evaluation with dynamic gadolinium-enhanced MR imaging. Radiology 1995; 194: pp. 529-536.
2. Puhakka K.B., Jurik A.G., Egund N., et. al.: Imaging of sacroiliitis in early seronegative spondyloarthropathy. Acta Radiol 2003; 44: pp. 218-229.
3. Pereira P.L., Gunaydin I., Trübenbach J., et. al.: Interventional MR imaging for injection of sacroiliac joints in patients with sacroiliitis. Am J Roentgenol AJR 2000; 175: pp. 265-266.
4. Jee W.H., McCauley T.R., Lee S.H., et. al.: Sacroiliitis in patients with ankylosing spondylitis: association of MR findings with disease activity. Magnet Reson Imaging 2004; 22: pp. 245-250.
5. Murphey M.D., Wetzel L.H., Bramble J.M., et. al.: Sacroiliitis: MR imaging findings. Radiology 1991; 180: pp. 239-244.
6. Yu W., Feng F., Dion E., et. al.: Comparison of radiography, computed tomography and magnetic resonance imaging in the detection of sacroiliitis accompanying ankylosing spondylitis. Skel Radiol 1998; 27: pp. 311-320.
7. Algin O., Gokalp G., Baran B., et. al.: Evaluation of sacroiliitis: contrast-enhanced MRI with subtraction technique. Skel Radiol 2009; 38: pp. 983-988.
8. Docherty P., Mitchell M.J., MacMillan L., et. al.: Magnetic resonance imaging in the detection of sacroiliitis. J Rheumatol 1992; 19: pp. 393-401.
9. Schaefer F.K., Kurz B., Schaefer P.J., et. al.: Accuracy and precision in the detection of articular cartilage lesions using resonance imaging at 1.5 tesla in an in vitro study with orthopedic and histopathologic correlation. Acta Radiol 2007; 48: pp. 1131-1137.
10. Verstraete K.L., Almqvist F., Verdonk P., et. al.: Magnetic resonance imaging of cartilage and cartilage repair. Clin Radiol 2004; 59: pp. 674-689.
11. Eckstein F., Hudelmaier M., Wirth W., et. al.: Double echo steady state magnetic resonance imaging of knee articular cartilage at 3 Tesla: a pilot study for the Osteoarthritis Initiative. Ann Rheum Dis 2006; 65: pp. 433-441.
12. Puhakka K.B., Melsen F., Jurik A.G., et. al.: MR imaging of the normal sacroiliac joint with correlation to histology. Skel Radiol 2004; 33: pp. 15-28.
13. Braun J., Sieper J., Bollow M.: Imaging of sacroiliitis. Clin Rheumatol 2000; 19: pp. 51-57.
14. Bredella M.A., Steinbach L.S., Morgan S., et. al.: MRI of the sacroiliac joints in patients with moderate to severe ankylosing spondylitis. Am J Roentgenol AJR 2006; 187: pp. 1420-1426.
15. Puhakka K.B., Jurik A.G., Schiottz-Christensen B., et. al.: Magnetic resonance imaging of sacroiliitis in early seronegative spondyloarthropathy. Abnormalities correlated to clinical and laboratory findings. Rheumatology 2004; 43: pp. 234-237.
16. Jeffrey D.R., Watt I.: Imaging hyaline cartilage. Br J Radiol 2003; 76: pp. 777-787.
17. Wittram C., Whitehouse G.H., Williams J.W., et. al.: A Comparison of MR and CT in suspected sacroiliitis. J Comp Assist Tomogr 1996; 20: pp. 68-72.
18. Boyle G.E., Ahern M., Cooke J., et. al.: An interactive taxonomy of MR imaging sequences. Radiographics 2006; 26: e24
19. Murphy B.J.: Evaluation of grades 3 and 4 chondromalacia of the knee using T2 ∗ -weighted 3D gradient echo articular cartilage imaging. Skel Radiol 2001; 30: pp. 305-311.
20. Ruehm S., Zanetti M., Romero J., et. al.: MRI of patellar articular cartilage: evaluation of an optimized gradient echo sequence (3D-DESS). J Magn Reson Imaging 1998; 8: pp. 1246-1251.