
Rationale and Objectives
To evaluate knowledge-based iterative model reconstruction (IMR) to improve image quality and reduce radiation dose in coronary computed tomography angiography (cCTA).
Materials and Methods
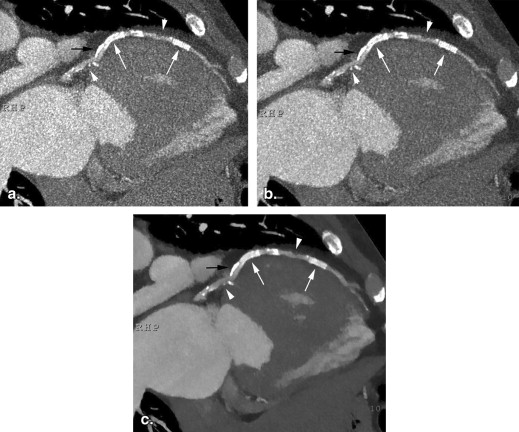
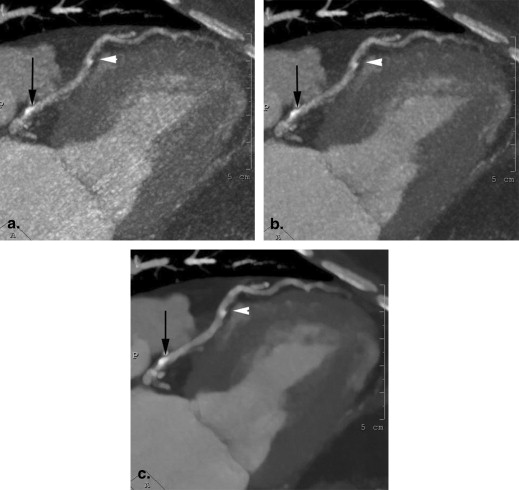
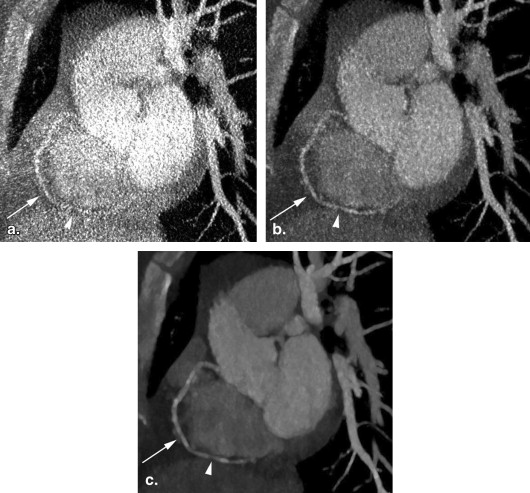
We evaluated 45 consecutive cCTA studies, including 25 studies performed with an 80% systolic dose reduction using tube current modulation (TCM). Each study was reconstructed with filtered back projection (FBP), hybrid iterative reconstruction (iDose 4 ), and IMR in a diastolic phase. Additional systolic phase reconstructions were obtained for TCM studies. Mean pixel attenuation value and standard deviation (SD) were measured in the left ventricle and left main coronary artery. Subjective scores were obtained by two independent reviewers on a 5-point scale for definitions of contours of small coronary arteries (<3 mm), coronary calcifications, noncalcified plaque, and overall diagnostic confidence for the presence/absence of stenosis.
Results
There was no significant difference in pixel intensity among FBP, iDose 4 , and IMR ( P > .8). For diastolic phase images, noise amplitude in the left main coronary artery was reduced by a factor of 1.3 from FBP to iDose 4 (SD = 99 vs. 74; P = .005) and by a factor of 2.6 from iDose 4 to IMR (SD = 74 vs. 28; P < .001). For systolic phase TCM images, noise amplitude in the left main coronary artery was reduced by a factor of 2.3 from FBP to iDose 4 (SD = 322 vs. 142; P < .001) and by a factor of 3.0 from iDose 4 to IMR (SD = 142 vs. 48; P < .001). All four subjective image quality scores were significantly better with IMR compared to iDose 4 and FBP ( P < .001). The reduction in image noise amplitude and improvement in image quality scores were greatest among obese patients.
Conclusions
IMR reduces intravascular noise on cCTA by 86%–88% compared to FBP, and improves image quality at radiation exposure levels 80% below our standard technique.
Since the introduction of the EMI computed tomography (CT) scanner in 1971, clinical CT image reconstruction has been based on filtered back projection (FBP) to reconstruct two-dimensional images from x-ray attenuation measurements in multiple one-dimensional planes. The original EMI scanner did provide an option for iterative reconstruction, but iterative reconstruction was not applied to clinical CT until recently because of computational requirements. Increased computational power now allows the application of iterative reconstruction techniques that were developed for lower resolution nuclear medicine images to high resolution CT. A history of CT reconstruction along with a synopsis of newer iterative reconstruction techniques are summarized in a recent review .
The first commercially available iterative reconstruction systems for CT used hybrid methods that combined FBP with iterative reconstruction to provide noise reduction. This noise reduction can be leveraged to improve image quality or to compensate for high noise with lower tube current acquisitions. Adaptive statistical iterative reconstruction (GE Healthcare, Waukesha, WI) and iDose 4 (Philips Healthcare, Cleveland, OH) are examples of this approach. These techniques decrease the noise in reconstructed images compared to FBP. Model-based iterative reconstruction by GE Healthcare and iterative model reconstruction (IMR) by Philips are the latest generation of commercially available iterative techniques that rely on statistical and system models and approach reconstruction as an optimization process. These newer techniques may simultaneously provide further reduction in image noise, potential dose savings, and improved image quality.
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diastolic Phase Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Image Noise within the Left Ventricle and Left Main Coronary Artery, Expressed as Standard Deviation within a Region of Interest for Diastolic Phase Reconstructions
FBP iDose 4 IMR Left ventricular noise1238217 Normal weight subgroup 96 71 14 Overweight subgroup 121 87 19 Obese subgroup 141 81 16 Left main coronary noise997428 Normal weight subgroup 86 66 36 Overweight subgroup 109 81 23 Obese subgroup 95 69 23
Numbers provided in bold font represent overall values for each group. Numbers in non-bold font are values for the individual subgroups.
Table 2
Subjective Image Quality Scores for Diastolic Phase Reconstructions on a 1–5 Scale Described in the Methods Section
FBP iDose 4 IMR Arterial contour2.13.24.8 Normal weight subgroup 2.8 3.8 5.0 Overweight subgroup 2.2 3.2 5.0 Obese subgroup 1.5 2.9 4.6 Coronary calcifications2.23.34.9 Normal weight subgroup 2.8 3.8 5.0 Overweight subgroup 2.2 3.4 5.0 Obese subgroup 1.5 2.6 4.6 Noncalcified plaque contour1.72.84.4 Normal weight subgroup 2.0 3.0 4.5 Overweight subgroup 2.2 3.2 4.6 Obese subgroup 1.1 2.4 4.3 Overall diagnostic confidence2.63.84.9 Normal weight subgroup 3.0 4.0 5.0 Overweight subgroup 2.6 3.8 5.0 Obese subgroup 2.0 3.6 4.8
Numbers provided in bold font represent overall values for each group. Numbers in non-bold font are values for the individual subgroups.
Get Radiology Tree app to read full this article<
Systolic Phase Imaging with TCM
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Subjective Image Quality Scores for Systolic Phase Reconstructions on a 1–5 Scale Described in the Methods Section
FBP iDose 4 IMR Arterial contour 1.6 2.7 4.5 Coronary calcifications 1.6 2.8 4.6 Noncalcified plaque contour 1.6 2.6 4.0 Overall diagnostic confidence 1.7 3.0 4.5
Get Radiology Tree app to read full this article<
Inter-rater Agreement
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Singh S., Khawaja R.D., Pourjabbar S., et. al.: Iterative image reconstruction and its role in cardiothoracic computed tomography. J Thorac Imaging 2013; 28: pp. 355-367.
2. Marin D., Nelson R.C., Schindera S.T., et. al.: Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm—initial clinical experience. Radiology 2010; 254: pp. 145-153.
3. Singh S., Kalra M.K., Hsieh J., et. al.: Abdominal CT: comparison of adaptive statistical iterative and filtered back projection reconstruction techniques. Radiology 2010; 257: pp. 373-383.
4. Noël P.B., Fingerle A.A., Renger B., et. al.: Initial performance characterization of a clinical noise-suppressing reconstruction algorithm for MDCT. AJR Am J Roentgenol 2011; 197: pp. 1404-1409.
5. Hou Y., Liu X., Xv S., et. al.: Comparisons of image quality and radiation dose between iterative reconstruction and filtered back projection reconstruction algorithms in 256-MDCT coronary angiography. AJR Am J Roentgenol 2012; 199: pp. 588-594.
6. Shuman W.P., Green D.E., Busey J.M., et. al.: Model-based iterative reconstruction versus adaptive statistical iterative reconstruction and filtered back projection in liver 64-MDCT: focal lesion detection, lesion conspicuity, and image noise. AJR Am J Roentgenol 2013; 200: pp. 1071-1076.
7. Volders D., Bols A., Haspeslagh M., et. al.: Model-based iterative reconstruction and adaptive statistical iterative reconstruction techniques in abdominal CT: comparison of image quality in the detection of colorectal liver metastases. Radiology 2013; 269: pp. 469-474.
8. Mayo J.R., Leipsic J.A.: Radiation dose in cardiac CT. AJR Am J Roentgenol 2009; 192: pp. 646-653.
9. Halpern E.J.: Technique, protocols, instrumentation, and radiation dose.Halpern E.J.Clinical cardiac CT—anatomy and function.2011.ThiemeNew York, NY:pp. 24-46.
10. Renker M., Geyer L.L., Kranzinski A.W., et. al.: Iterative image reconstruction: a realistic dose-saving method in cardiac CT imaging?. Expert Rev Cardiovasc Ther 2013; 11: pp. 403-409.
11. Fleiss J.L., Cohen J.: The equivalence of weighted kappa and the intraclass correlation coefficient as measures of reliability. Educ Psychol Meas 1973; 33: pp. 613-619.
12. Oda S., Utsunomiya D., Funama Y., et. al.: A knowledge-based iterative model reconstruction algorithm: can super-low-dose cardiac CT be applicable in clinical settings?. Acad Radiol 2014; 21: pp. 104-110.
13. Lee C.H., Goo J.M., Ye H.J., et. al.: Radiation dose modulation techniques in the multidetector CT era: from basics to practice. Radiographics 2008; 28: pp. 1451-1459.
14. McCollough C.H., Primak A.N., Braun N., et. al.: Strategies for reducing radiation dose in CT. Radiol Clin North Am 2009; 47: pp. 27-40.
15. Menke J.: Comparison of different body size parameters for individual dose adaptation in body CT of adults. Radiology 2005; 236: pp. 565-571.
16. Mulkens T.H., Bellinck P., Baeyaert M., et. al.: Use of an automatic exposure control mechanism for dose optimization in multi-detector row CT examinations: clinical evaluation. Radiology 2005; 237: pp. 213-223.
17. Leipsic J., Labounty T.M., Heilbron B., et. al.: Adaptive statistical iterative reconstruction: assessment of image noise and image quality in coronary CT angiography. AJR Am J Roentgenol 2010; 195: pp. 649-654.
18. Solomon J.B., Christianson O., Samei E.: Quantitative comparison of noise texture across CT scanners from different manufacturers. Med Phys 2012; 39: pp. 6048-6055.