
Rationale and Objectives
Milan criteria recommends selection of candidates with hepatocellular carcinoma (HCC) for liver transplantation based on strict tumor size thresholds. The purpose of this study is to compare the effect of two-dimensional and three-dimensional tumor measurements on the selection of candidates for liver transplantation using Milan criteria.
Materials and Methods
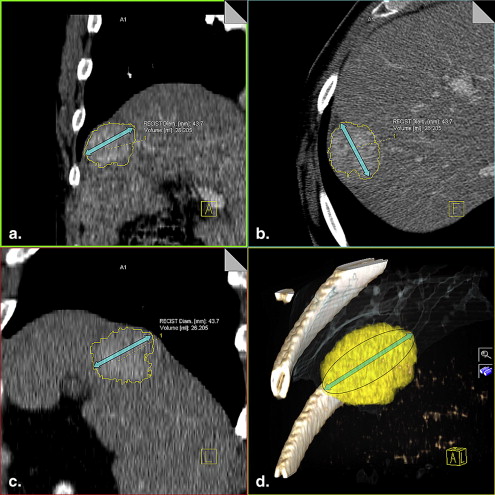
This retrospective Health Insurance Portability and Accountability Act–compliant study was approved by our institutional review board. Patient-informed consent was waived. Forty-five HCCs in 19 patients, evaluated with triphasic multidetector row computed tomography scans, were included in the analysis. The largest diameters in each two-dimensional orthogonal plane (Max2D) and within three-dimensional tumor boundaries (Max3D) were calculated for each lesion. Diameters were compared and the eligibility based on lesion size for liver transplantation was assessed.
Results
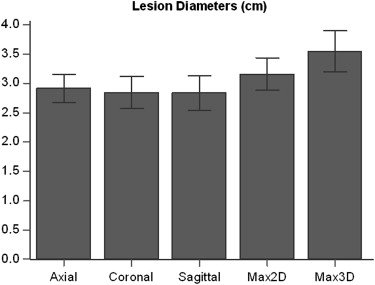
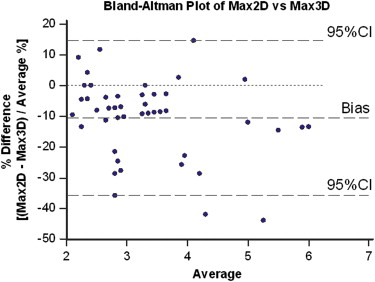
The mean Max2D diameter of HCC was 3.2 ± 0.9 cm and the mean Max3D diameter was 3.5 ± 1.2 cm. There was a significant difference between the mean Max2D and Max3D diameters ( P < .001). Among the 45 lesions, 22 of them (48.9%) were ineligible for transplantation according to Max2D diameter, whereas 29 of them (64.44%) were ineligible when Max3D diameter was applied ( P < .001).
Conclusion
HCC diameter based on 3D measurements is significantly different than the conventional 2D measurements and may affect eligibility for liver transplantation.
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver, and its incidence has been rising in the past two decades. Curative treatments such as surgical resection and transplantation may be only indicated in patients with small tumors .
Since the beginning of the technical development of liver transplantation, nonresectable malignant lesions have been considered as a possible indication for transplantation. However, it has been recognized that patients with large, multiple, or widespread hepatocellular carcinomas with vascular invasion or extrahepatic involvement have a poor prognosis in terms of survival and recurrence, whereas patients with small, incidental tumors had the same outcome as patients transplanted for other reasons .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Patients
Get Radiology Tree app to read full this article<
Imaging Technique
Get Radiology Tree app to read full this article<
Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kaseb A.O., Hanbali A., Cotant M., et. al.: Vascular endothelial growth factor in the management of hepatocellular carcinoma: a review of literature. Cancer 2009; 115: pp. 4895-4906.
2. Bruix J., Sherman M.: Management of hepatocellular carcinoma. Hepatology 2005; 42: pp. 1208-1236.
3. Bruix J., Fuster J., Llovet J.M.: Liver transplantation for hepatocellular carcinoma: Foucault pendulum versus evidence-based decision. Liver Transpl 2003; 9: pp. 700-702.
4. Mazzaferro V., Regalia E., Doci R., et. al.: Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. New Engl J Med 1996; 334: pp. 693-699.
5. Yao F.Y., Ferrell L., Bass N.M., et. al.: Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology 2001; 33: pp. 1394-1403.
6. Freeman R.B., Wiesner R.H., Harper A., et. al.: The new liver allocation system: moving toward evidence-based transplantation policy. Liver Transpl 2002; 8: pp. 851-858.
7. Suzuki C., Jacobsson H., Hatschek T., et. al.: Radiologic measurements of tumor response to treatment: practical approaches and limitations. Radiographics 2008; 28: pp. 329-344.
8. Kelsey C.R., Schefter T., Nash S.R., et. al.: Retrospective clinicopathologic correlation of gross tumor size of hepatocellular carcinoma: implications for stereotactic body radiotherapy. Am J Clin Oncol 2005; 28: pp. 576-580.
9. Bornemann L., Kuhnigk J.M., Dicken V., et. al.: Informatics in radiology (infoRAD): new tools for computer assistance in thoracic CT part 2. Therapy monitoring of pulmonary metastases. Radiographics 2005; 25: pp. 841-848.
10. Kuhnigk J.M., Dicken V., Bornemann L., et. al.: Morphological segmentation and partial volume analysis for volumetry of solid pulmonary lesions in thoracic CT scans. IEEE Trans Med Imaging 2006; 25: pp. 417-434.
11. Keil S., Behrendt F.F., Stanzel S., et. al.: Semi-automated measurement of hyperdense, hypodense and heterogeneous hepatic metastasis on standard MDCT slices. Comparison of semi-automated and manual measurement of RECIST and WHO criteria. Eur Radiol 2008; 18: pp. 2456-2465.
12. Moltz J.H., Bornemann L., Kuhnigk J.M., et. al.: Advanced segmentation techniques for lung nodules, liver metastases, and enlarged lymph nodes in CT scans. IEEE J Sel Top Signal Process 2009; 3: pp. 122-134.
13. Bornemann L., Dicken V., Kuhnigk J.M., et. al.: OncoTREAT: a software assistant for cancer therapy monitoring. Int J CARS 2007; 1: pp. 231-242.
14. Marchiano A., Calabro E., Civelli E., et. al.: Pulmonary nodules: volume repeatability at multidetector CT lung cancer screening. Radiology 2009; 251: pp. 919-925.
15. Bruix J., Sherman M., Llovet J.M., et. al.: Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol 2001; 35: pp. 421-430.
16. Huang J.S., Pan H.B., Chou C.P., et. al.: Optimizing scanning phases in detecting small (<2 cm) hepatocellular carcinoma: whole-liver dynamic study with multidetector row CT. J Comput Assist Tomogr 2008; 32: pp. 341-346.
17. Ichikawa T., Kitamura T., Nakajima H., et. al.: Hypervascular hepatocellular carcinoma: can double arterial phase imaging with multidetector CT improve tumor depiction in the cirrhotic liver?. AJR Am J Roentgenol 2002; 179: pp. 751-758.
18. Roayaie K., Feng S.: Allocation policy for hepatocellular carcinoma in the MELD era: room for improvement?. Liver Transpl 2007; 13: pp. S36-S43.
19. Weismüller T.J., Fikatas P., Schmidt J., et. al.: Multicentric evaluation of model for end-stage liver disease-based allocation and survival after liver transplantation in Germany—limitations of the ‘sickest first’-concept. Transplant Intl 2011; 24: pp. 91-99.
20. Thuluvath P.J., Guidinger M.K., Fung J.J., et. al.: Liver transplantation in the United States, 1999–2008. Am J Transplant 2010; 10: pp. 1003-1019.
21. Freeman R.B., Mithoefer A., Ruthazer R., et. al.: Optimizing staging for hepatocellular carcinoma before liver transplantation: a retrospective analysis of the UNOS/OPTN database. Liver Transpl 2006; 12: pp. 1504-1511.
22. Pawlik T.M., Delman K.A., Vauthey J.N., et. al.: Tumor size predicts vascular invasion and histologic grade: implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transpl 2005; 11: pp. 1086-1092.
23. Yao F.Y., Ferrell L., Bass N.M., et. al.: Liver transplantation for hepatocellular carcinoma: comparison of the proposed UCSF criteria with the Milan criteria and the Pittsburgh modified TNM criteria. Liver Transpl 2002; 8: pp. 765-774.
24. Botea F., Marconi M., Lutman F., et. al.: Radiological estimation of size in colorectal liver metastases: is it reliable? Comparison with post-resectional measurements. Updates Surg 2010; 62: pp. 21-26.
25. Mantatzis M., Kakolyris S., Amarantidis K., et. al.: Treatment response classification of liver metastatic disease evaluated on imaging. Are RECIST unidimensional measurements accurate?. Eur Radiol 2009; 19: pp. 1809-1816.
26. Sohaib S.A., Turner B., Hanson J.A., et. al.: CT assessment of tumour response to treatment: comparison of linear, cross-sectional and volumetric measures of tumour size. Br J Radiol 2000; 73: pp. 1178-1184.
27. Dubus L., Gayet M., Zappa M., et. al.: Comparison of semi-automated and manual methods to measure the volume of liver tumours on MDCT images. Eur Radiol 2011; 21: pp. 996-1003.
28. Jaffe C.C.: Measures of response: RECIST, WHO, and new alternatives. J Clin Oncol 2006; 24: pp. 3245-3251.
29. Zimmerman M.A., Ghobrial R.M., Tong M.J., et. al.: Recurrence of hepatocellular carcinoma following liver transplantation: a review of preoperative and postoperative prognostic indicators. Arch Surg 2008; 143: pp. 182-188.
30. Hwang S., Ahn C.S., Kim K.H., et. al.: Super-selection of a subgroup of hepatocellular carcinoma patients at minimal risk of recurrence for liver transplantation. J Gastrointest Surg 2011; 15: pp. 971-981.
31. Miller A.B., Hoogstraten B., Staquet M., et. al.: Reporting results of cancer treatment. Cancer 1981; 47: pp. 207-214.
32. Buerke B., Puesken M., Beyer F., et. al.: Semiautomatic lymph node segmentation in multislice computed tomography: impact of slice thickness on segmentation quality, measurement precision, and interobserver variability. Invest Radiol 2010; 45: pp. 82-88.