
The American College of Radiology (ACR) Appropriateness Criteria was compiled as a set of evidence-based guidelines to aid both radiologists and referring physicians in making efficient use of imaging resources. In our study, only 60% of residents knew how to obtain a copy of the ACR Appropriateness Criteria, and 90% were unaware of its contents. The overall mean score in a Medical Decision Support Competency Quiz was less than 60%. We propose that there is a clear need for the formal implementation of the ACR Appropriateness Criteria within our radiology training programs. Residents should be better familiarized with its contents so as to improve medical decision support to clinicians, technologists, and radiologists alike.
With rapidly growing health care and imaging costs, it has become necessary for radiologists to play an integral role in assisting referring physicians in making cost effective decisions with respect to imaging studies for their patients. Today’s changing health care environment further highlights the need to address this issue, not only for improved patient care, but also for the obvious financial impacts on health care institutions across the United States. As imaging volumes increase, there will be greater pressure placed on all physicians to justify each imaging study. In 1993, the leadership of the American College of Radiology (ACR) decided that an institution of nationally accepted, evidence-based guidelines was necessary to assist radiologists and referring physicians . Today, the ACR Appropriateness Criteria exists as an easily accessible document for the purpose of enhancing medical imaging decision support. In one cohort of trauma patients who underwent computed tomography (CT) scans, it was suggested that nearly 44% of the overall radiation dose and approximately 39% of the total fees incurred could have been avoided if the ACR criteria were used . Over the past few years, an increased number of inpatient institutions have adopted the predominant use of hospitalists rather than primary care physicians with inpatient privileges, with several articles reporting resultant improved efficiency in patient care . Although hospitalists decrease health care costs, they do so by reducing length of stay and not by reducing imaging costs. This is described in a study by Khasgiwala et al , in which hospitalists demonstrated no reduction in imaging utilization compared to their non-hospitalist counterparts. This hospitalist approach to inpatient care closely parallels the structure of university hospitals with resident physicians. A significant proportion of imaging decision support is sought after hours, from the on-call radiology resident. The resident must be able to provide evidence-based decision support, or at the very least, know where to find the necessary information. Our goal in this study is to evaluate the familiarity of the radiology residents in our institution with the ACR Appropriateness Criteria within the realm of musculoskeletal (MSK) radiology, and to evaluate their ability to apply this knowledge within the context of imaging decision support.
Methods
A 23-item multiple-choice and true-false Imaging Decision-Management Scenario Quiz was created based on the MSK Section of the ACR Appropriateness Criteria. This quiz was given in an impromptu manner to all available radiology residents in our institution to evaluate not only their knowledge but also their ability to use the contents of these criteria within the context of imaging decision support. Specific Imaging Management Categories included: hardware, infection, tumor, trauma, pain, and other (bone mineral density and radiation physics) with specific questions regarding familiarity and knowledge of the ACR criteria, as well as frequency of utilization of medical decision support resources in training. Year of training was recorded. All quizzes were evaluated by two radiologists. Sample questions included the following.
1. Based on several studies, it is now evident that uncomplicated acute low back pain or radiculopathy is a benign, self-limited condition that does not warrant any imaging studies. Which of the following DOES NOT constitute a “red flag,” indicating a potentially more complicated scenario?
a. Age >70 years.
b. History of intravenous drug use.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Residents’ Performance on the Overall Medical Decision Support Competency Test and Specific Decision Categories
Test Categories n Mean Score Standard Deviation Overall percentage of correct decisions 20 54.75 14.46 Bone tumor management 20 49.20 21.29 Trauma management 20 57.00 23.64 Infection management 20 46.60 22.91 Orthopedic hardware management 20 52.50 30.24 Non–trauma-related pain management 20 64.37 18.71 Other (bone mineral density and radiation physics) 20 35.00 36.63
Table 2
Percentage of Correct Decisions by Residency Year
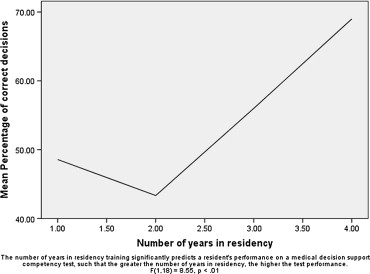
Number of Years in Residency Mean n Standard Deviation 1 48.57 7 12.15 2 43.33 3 10.41 3 56.00 5 11.40 4 69.00 5 12.94 All years 54.75 20 14.46
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
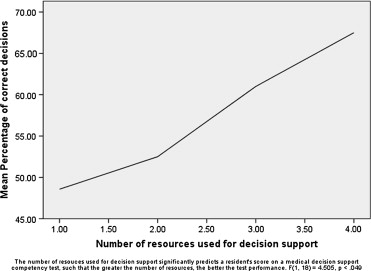
Residents’ Frequency in Using Various Medical Decision Support Resources
Response Options Educated Guess, Based on Rotation Experience Ask Attending Ask Technician Use search Engine Use Knowledge Obtained from the American College of Cardiology Criteria Frequency 10 18 5 9 1
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. ACR Appropriateness Criteria Background and Development. Available online at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/BackgroundandDevelopment.aspx . Accessed February 05, 2009.
2. Hadley J.L., Agola J., Wong P.: Potential impact of the American College of Radiology appropriateness criteria on CT for trauma. AJR Am J Roentgenol 2006; 186: pp. 937-942.
3. Khasgiwala V.C., Aronson M.D., Davis R.B., et. al.: Imaging utilization in the era of the hospitalist. AJR Am J Roentgenol 2006; 187: pp. 2-7.
4. Khorasani R.: Computerized physician order entry and decision support: improving the quality of care. RadioGraphics 2001; 21: pp. 1015-2101.
5. Blackmore C.C., Medina S.L.: Evidence-based radiology and the ACR appropriateness criteria. J Am Coll Radiol 2006; 3: pp. 505-509.
6. Jamal T., Gunderman R.B.: The American College of Radiology Appropriateness Criteria: the user’s perspective. J Am Coll Radiol 2008; 5: pp. 158-216.
7. Gunderman R.B., Bettmann M., Davis L.P.: Promoting educational innovation: lessons from the request for proposals for ACR appropriateness criteria usage in medical education. J Am Coll Radiol 2007; 4: pp. 919-924.