
Rationale and Objectives
The characterization of plaques based on their computed tomography (CT) number is important for the detection of vulnerable atherosclerotic plaques. An earlier in vitro study showed that intravascular attenuation affected the attenuation of coronary atherosclerotic plaques. We attempted to validate this finding in vivo and here we introduce a dual-phase coronary CT angiography (CCTA) technique to address this issue.
Materials and Methods
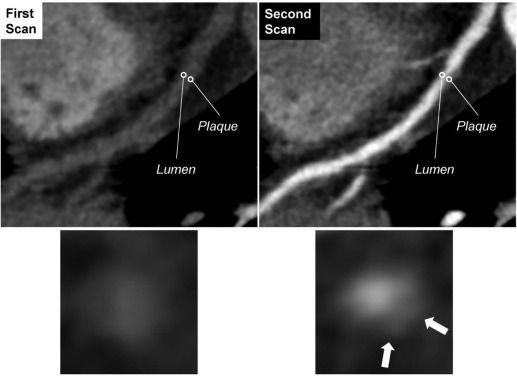
Institutional ethics committee approval and informed consent were obtained. Thirty patients (30 noncalcified plaques) underwent dual-phase CCTA. Two CT datasets were obtained, one with coronary artery enhancement and the other without coronary artery enhancement. The CT number of the plaque and the adjacent vessel lumen was measured in a circular region of interest on curved planar reconstruction images. The region of interest setting was consistent between the two CT datasets. We performed linear regression analysis of the changes in the CT numbers (ΔHounsfield unit), calculated by subtracting the two CT datasets, for the lumen and for the plaque. We also evaluated the relationship between plaque attenuation on nonenhanced coronary artery images and luminal attenuation with and without contrast enhancement.
Results
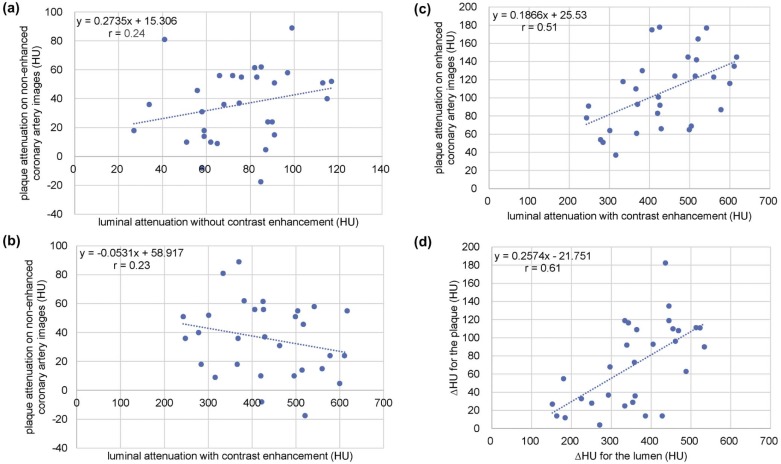
The ΔHounsfield unit for the plaque and the lumen showed a strong correlation (r = 0.61). There was no significant correlation between plaque attenuation on nonenhanced coronary artery images and luminal attenuation with and without contrast enhancement (r = 0.23 and 0.24, respectively).
Conclusions
Intravascular attenuation changed the attenuation of coronary atherosclerotic plaques. Using the copy-paste technique, the CT number of identical plaques can be measured in registered dual-phase CCTA images for the evaluation of coronary plaques.
Introduction
Coronary computed tomography angiography (CCTA) has shown good potential for the detection, quantification, and characterization of coronary artery plaques . However, a previous phantom study reported that the increased attenuation of the contrast material in a silicon coronary artery phantom determined an increase in the measured attenuation of the plaque made of rubber material . In a human ex vivo study , coronary lumen attenuation affected the attenuation values used to define the composition of coronary plaques. These findings have not been fully validated in vivo and the best scanning protocol for the identification and the characterization of noncalcified plaques remains to be established.
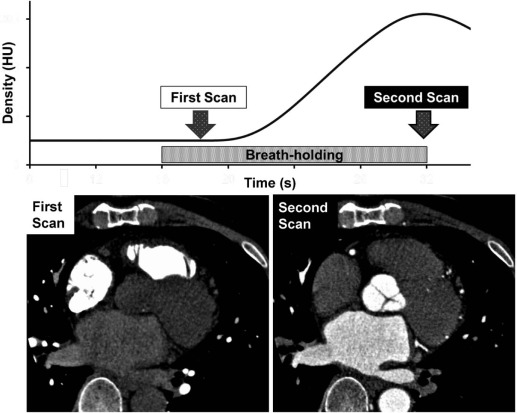
The 320-row CT scanners combine faster gantry rotation (0.275 seconds) and wide volume coverage (16 cm) . They make it possible to perform two consecutive (dual-phase) CCTA at the same electrocardiogram (ECG) phase but at different heartbeats in a single breath-hold without having to move the patient. In dual-phase CCTA, two CT datasets (one with contrast enhancement and the other without contrast enhancement in the coronary arteries) can be obtained by optimization of the first- and the second-phase scan timing . As two acquisitions are performed at the same anatomic location, the two CT datasets can be registered accurately with dedicated application software . Consequently, the CT number of identical noncalcified plaques can be measured on nonenhanced and enhanced coronary artery images using the copy-paste technique, and the relationship between plaque attenuation and coronary artery enhancement can be determined.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
CT Scanning and Contrast Infusion Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Image Quality Analysis
Get Radiology Tree app to read full this article<
CT Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Summary of the Attenuation Values Measured on Dual-phase Scans
Number First Phase Second Phase_P_ Value Lumen 30 75 ± 23 HU 435 ± 110 HU <0.01 Plaque 30 36 ± 25 HU 107 ± 40 HU <0.01
HU, Hounsfield unit.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kopp A.F., Schroeder S., Baumbach A., et. al.: Non-invasive characterisation of coronary lesion morphology and composition by multislice CT: first results in comparison with intracoronary ultrasound. Eur Radiol 2001; 11: pp. 1607-1611.
2. Leber A.W., Knez A., Becker A., et. al.: Accuracy of multidetector spiral computed tomography in identifying and differentiating the composition of coronary atherosclerotic plaques: a comparative study with intracoronary ultrasound. J Am Coll Cardiol 2004; 43: pp. 1241-1247.
3. Nakazato R., Shalev A., Doh J.H., et. al.: Quantification and characterisation of coronary artery plaque volume and adverse plaque features by coronary computed tomographic angiography: a direct comparison to intravascular ultrasound. Eur Radiol 2013; 23: pp. 2109-2117.
4. Kimura S., Yonetsu T., Suzuki K., et. al.: Characterisation of non-calcified coronary plaque by 16-slice multidetector computed tomography: comparison with histopathological specimens obtained by directional coronary atherectomy. Int J Cardiovasc Imaging 2012; 28: pp. 1749-1762.
5. Schroeder S., Kuettner A., Leitritz M., et. al.: Reliability of differentiating human coronary plaque morphology using contrast-enhanced multislice spiral computed tomography: a comparison with histology. J Comput Assist Tomogr 2004; 28: pp. 449-454.
6. de Weert T.T., Ouhlous M., Meijering E., et. al.: In vivo characterization and quantification of atherosclerotic carotid plaque components with multidetector computed tomography and histopathological correlation. Arterioscler Thromb Vasc Biol 2006; 26: pp. 2366-2372.
7. Schroeder S., Flohr T., Kopp A.F., et. al.: Accuracy of density measurements within plaques located in artificial coronary arteries by X-ray multislice CT: results of a phantom study. J Comput Assist Tomogr 2001; 25: pp. 900-906.
8. Cademartiri F., Mollet N.R., Runza G., et. al.: Influence of intracoronary attenuation on coronary plaque measurements using multislice computed tomography: observations in an ex vivo model of coronary computed tomography angiography. Eur Radiol 2005; 15: pp. 1426-1431.
9. Oda S., Utsunomiya D., Yuki H., et. al.: Low contrast and radiation dose coronary CT angiography using a 320-row system and a refined contrast injection and timing method. J Cardiovasc Comput Tomogr 2015; 9: pp. 19-27.
10. Funama Y., Utsunomiya D., Taguchi K., et. al.: Automatic exposure control at single- and dual-heartbeat CTCA on a 320-MDCT volume scanner: effect of heart rate, exposure phase window setting, and reconstruction algorithm. Phys Med 2014; 30: pp. 385-390.
11. Kidoh M., Utsunomiya D., Oda S., et. al.: Optimized subtraction coronary CT angiography protocol for clinical use with short breath-holding time-initial experience. Acad Radiol 2015; 22: pp. 117-120.
12. Yoshioka K., Tanaka R., Muranaka K.: Subtraction coronary CT angiography for calcified lesions. Cardiol Clin 2012; 30: pp. 93-102.
13. Tanaka R., Yoshioka K., Muranaka K., et. al.: Improved evaluation of calcified segments on coronary CT angiography: a feasibility study of coronary calcium subtraction. Int J Cardiovasc Imaging 2013; 29: pp. 75-81.
14. Yoshioka K., Tanaka R., Muranaka K., et. al.: Subtraction coronary CT angiography using second-generation 320-detector row CT. Int J Cardiovasc Imaging 2015; 31: pp. 51-58.
15. Bedayat A., Rybicki F.J., Kumamaru K., et. al.: Reduced exposure using asymmetric cone beam processing for wide area detector cardiac CT. Int J Cardiovasc Imaging 2012; 28: pp. 381-388.
16. Van der Molen A.J., Joemai R.M., Geleijns J.: Performance of longitudinal and volumetric tube current modulation in a 64-slice CT with different choices of acquisition and reconstruction parameters. Phys Med 2012; 28: pp. 319-326.
17. Jessen K.A., Shrimpton P.C., Geleijns J., et. al.: Dosimetry for optimisation of patient protection in computed tomography. Appl Radiat Isot 1999; 50: pp. 165-172.
18. Dalager M.G., Bottcher M., Andersen G., et. al.: Impact of luminal density on plaque classification by CT coronary angiography. Int J Cardiovasc Imaging 2011; 27: pp. 593-600.
19. Nakaura T., Kidoh M., Sakaino N., et. al.: Low contrast- and low radiation dose protocol for cardiac CT of thin adults at 256-row CT: usefulness of low tube voltage scans and the hybrid iterative reconstruction algorithm. Int J Cardiovasc Imaging 2013; 29: pp. 913-923.
20. Tanami Y., Ikeda E., Jinzaki M., et. al.: Computed tomographic attenuation value of coronary atherosclerotic plaques with different tube voltage: an ex vivo study. J Comput Assist Tomogr 2010; 34: pp. 58-63.
21. Fuchs A., Kuhl J.T., Chen M.Y., et. al.: Feasibility of coronary calcium and stent image subtraction using 320-detector row CT angiography. J Cardiovasc Comput Tomogr 2015; 9: pp. 393-398.
22. Amanuma M., Kondo T., Sano T., et. al.: Subtraction coronary computed tomography in patients with severe calcification. Int J Cardiovasc Imaging 2015; 31: pp. 1635-1642.