
Rationale and Objectives
There is lack of information on the learning curve and the effect of operator’s experience on the quality outcomes of transarterial hepatic embolization (TAE). The aim of this study was to evaluate the effect of operator experience on outcomes of TAE of hepatocellular carcinoma.
Materials and Methods
Demographic characteristics and outcomes including overall survival (OS), time to local tumor progression (TLP), and post-procedure complications in patients with hepatocellular carcinoma treated with TAE were collected. Operators’ experience was measured in years based on the years after completion of fellowship and the date of first embolization, and was divided into five groups: G1, less than 5 years of operator’s experience (YOE) at the time of first embolization; G2, 5–10 YOE; G3, 10–15 YOE; G4, 15–20 YOE; and G5, more than 20 YOE. The effects of operator’s experience and outcomes were assessed using linear regression.
Results
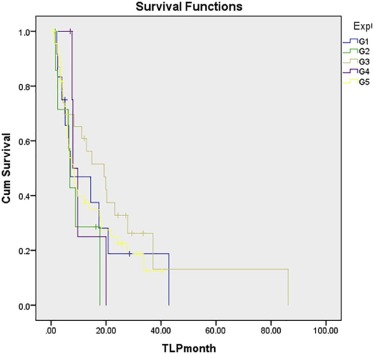
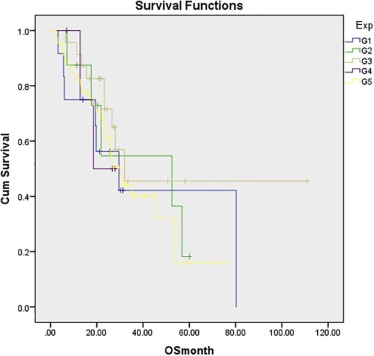
From January 2012 to January 2015, 93 patients (age range = 30–86 years) were treated. The number of patients treated by each group was as follows: G1 = 12; G2 = 8; G3 = 23; G4 = 5; and G5 = 45. All groups were similar in regard to degree of cirrhosis, Barcelona Clinic Liver Cancer staging, and Child-Pugh score ( P > .05). Median TLP was 8.8 months. TLP was 7.0, 6.8, 19.2, 7.9, and 8.2 months in G1, G2, G3, G4, and G5, respectively ( P = .56). OS for 1, 2, and 3 years was 75%, 56%, and 42% for G1; 87%, 54%, and 54% for G2; 91%, 71%, and 45% for G3, 100%, 50%, and 0 for G4; and 84%, 65%, and 40% for G5.
Conclusion
Among interventional radiology fellowship-trained operators in a tertiary cancer center, OS, TLP, and post-procedure complications of TAE were not affected by the years of post-fellowship experience.
Introduction
Transarterial hepatic embolization (TAE) and transarterial chemoembolization (TACE) are two minimally invasive procedures that interventional radiologists (IRs) have been using in the past 3–4 decades. Both procedures have been used extensively to treat nonsurgical patients with hepatocellular carcinoma (HCC) . TACE has been shown to be safe and effective in improving the overall survival (OS) when compared to best supportive care through randomized clinical trials . Most recently, in a randomized clinical trial, TAE was compared to doxorubicin-eluting microsphere chemoembolization and the study demonstrated that TAE was as effective and safe as the latter .
The principles of how to perform TAE and TACE are part of the teaching curriculum of any IR fellowship training program. The technical success in most interventions is related to skills that are obtained during training and continue to improve after finishing training and during independent practice. IR fellows are trained on how to use wires, microwires, catheters, and microcatheters. Additionally, IR fellows will get educated on principles of embolization and different embolizing options.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Patient Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Transarterial Hepatic Embolization Procedure
Get Radiology Tree app to read full this article<
Operator Experience
Get Radiology Tree app to read full this article<
Outcome
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Demographic Characteristic
Get Radiology Tree app to read full this article<
TABLE 1
Demographic Characteristics of the Five Groups of HCC Patients Treated With TAE
G1 G2 G3 G4 G5P__n 12 8 23 5 45 Age (y) 68.7 67.1 65.8 64.2 67.9 .891 Gender Female 2 0 7 2 15 .427 Male 10 8 16 3 30 Cirrhosis .504 No 3 3 7 0 9 Yes 9 5 16 5 36 Child-Pugh score .872 A 12 8 23 5 41 B 0 0 0 0 4 C 0 0 0 0 0 BCLC .833 A 3 2 9 1 16 B 6 4 10 4 18 C 3 2 4 0 11 % Liver involvement .789 <25% 7 6 15 4 28 >25, <50 5 1 5 1 15 >50, <75 0 1 2 0 2 >76–100 0 0 1 0 0 Extrahepatic disease .6 No 12 8 23 5 45 Yes 0 0 0 0 0 Previous surgery .060 Yes 5 4 12 1 9 No 7 4 11 4 36 ECOG .602 0 11 7 22 13 36 1 1 1 0 0 0 2 0 0 0 0 0 3 0 0 0 0 0 Systemic chemotherapy .366 No 11 6 22 5 42 Yes 1 2 1 0 3
BCLC, Barcelona Clinic Liver Cancer; ECOG, Eastern Corporative Oncology Group.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Technical Aspects
Get Radiology Tree app to read full this article<
Outcomes
Local Tumor Progression Free Survival
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Overall Survival
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Complications
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Marelli L., Stigliano R., Triantos C., et. al.: Transarterial therapy for hepatocellular carcinoma: which technique is more effective? A systematic review of cohort and randomized studies. Cardiovasc Intervent Radiol 2007; 30: pp. 6-25. PubMed PMID 17103105
2. Brown K.T., Do R.K., Gonen M., et. al.: Randomized trial of hepatic artery embolization for hepatocellular carcinoma using doxorubicin-eluting microspheres compared with embolization with microspheres alone. J Clin Oncol 2016; 34: pp. 2046-2053. PubMed PMID 26834067
3. Llovet J.M., Real M.I., Montana X., et. al.: Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet 2002; 359: pp. 1734-1739. PubMed PMID 12049862
4. Lee T.Y., Lin J.T., Ho H.J., et. al.: Evaluation of the effect of cumulative operator experience on hepatocellular carcinoma recurrence after primary treatment with radiofrequency ablation. Radiology 2015; 276: pp. 294-301. PubMed PMID 25763830
5. Poon R.T., Ng K.K., Lam C.M., et. al.: Learning curve for radiofrequency ablation of liver tumors: prospective analysis of initial 100 patients in a tertiary institution. Ann Surg 2004; 239: pp. 441-449. PubMed PMID 15024304 Pubmed Central PMCID: PMC1356248
6. Rege R.V., Joehl R.J.: A learning curve for laparoscopic splenectomy at an academic institution. J Surg Res 1999; 81: pp. 27-32. PubMed PMID 9889053
7. Maluccio M., Covey A.M., Gandhi R., et. al.: Comparison of survival rates after bland arterial embolization and ablation versus surgical resection for treating solitary hepatocellular carcinoma up to 7 cm. J Vasc Interv Radiol 2005; 16: pp. 955-961. PubMed PMID 16002503
8. Wojcik M., Berkowitsch A., Greis H., et. al.: Learning curve in cryoballoon ablation of atrial fibrillation: eight-year experience. Circ J 2014; 78: pp. 1612-1618. PubMed PMID 24837706
9. Lin D.Y., Liaw Y.F., Lee T.Y., et. al.: Hepatic arterial embolization in patients with unresectable hepatocellular carcinoma—a randomized controlled trial. Gastroenterology 1988; 94: pp. 453-456. PubMed PMID 2826285
10. Kawai S., Okamura J., Ogawa M., et. al.: Prospective and randomized clinical trial for the treatment of hepatocellular carcinoma—a comparison of lipiodol-transcatheter arterial embolization with and without adriamycin (first cooperative study). The Cooperative Study Group for Liver Cancer Treatment of Japan. Cancer Chemother Pharmacol 1992; 31: pp. S1-S6. PubMed PMID 1281041
11. Meyer T., Kirkwood A., Roughton M., et. al.: A randomised phase II/III trial of 3-weekly cisplatin-based sequential transarterial chemoembolisation vs embolisation alone for hepatocellular carcinoma. Br J Cancer 2013; 108: pp. 1252-1259. PubMed PMID 23449352 Pubmed Central PMCID: Pmc3619271
12. Parise P., Elmore U., Fumagalli U., et. al.: Esophageal surgery in Italy. Criteria to identify the hospital units and the tertiary referral centers entitled to perform it. Updates Surg 2016; 68: pp. 129-133. PubMed PMID 27240756
13. Birkmeyer J.D., Siewers A.E., Finlayson E.V., et. al.: Hospital volume and surgical mortality in the United States. N Engl J Med 2002; 346: pp. 1128-1137. PubMed PMID 11948273
14. O’Kane D., Papa N., Lawrentschuk N., et. al.: Supervisor volume affects oncological outcomes of trainees performing open radical prostatectomy. ANZ J Surg 2016; 86: pp. 249-254. PubMed PMID 25916513
15. Deschamps F., Solomon S.B., Thornton R.H., et. al.: Computed analysis of three-dimensional cone-beam computed tomography angiography for determination of tumor-feeding vessels during chemoembolization of liver tumor: a pilot study. Cardiovasc Intervent Radiol 2010; 33: pp. 1235-1242. PubMed PMID 20390271 Pubmed Central PMCID: PMC2977071
16. Miyayama S., Yamashiro M., Hashimoto M., et. al.: Identification of small hepatocellular carcinoma and tumor-feeding branches with cone-beam CT guidance technology during transcatheter arterial chemoembolization. J Vasc Interv Radiol 2013; 24: pp. 501-508. PubMed PMID 23452552
17. Carrafiello G., Ierardi A.M., Duka E., et. al.: Usefulness of cone-beam computed tomography and automatic vessel detection software in emergency transarterial embolization. Cardiovasc Intervent Radiol 2016; 39: pp. 530-537. PubMed PMID 26486155
18. Ronot M., Abdel-Rehim M., Hakime A., et. al.: Cone-beam CT angiography for determination of tumor-feeding vessels during chemoembolization of liver tumors: comparison of conventional and dedicated-software analysis. J Vasc Interv Radiol 2016; 27: pp. 32-38. PubMed PMID 26549371