
Rationale and Objectives
To investigate the correlation between prevalence and degree of coronary artery calcification (CAC) and extracoronary calcifications (ECCs), scored quantitatively according to Agatston and semiquantitatively by visual analysis, in chest computed tomography (CT) studies obtained for lung cancer screening in asymptomatic subjects and in patients with known coronary heart disease (CHD), and to compare the association of ECC and CAC to established cardiovascular risk factors.
Materials and Methods
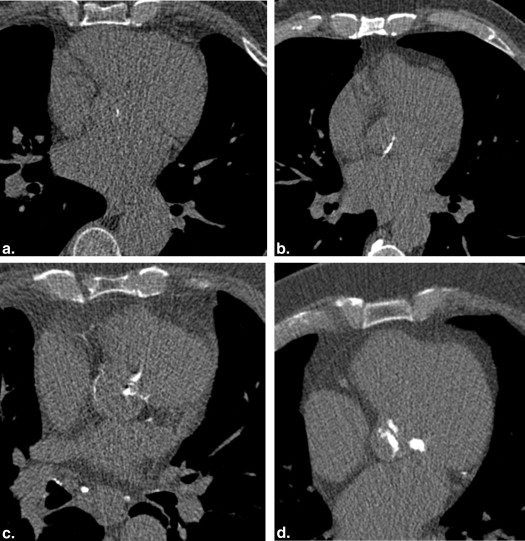
Prospective study on 501 males (67 ± 8 years) with a history of working dust exposure who underwent nongated low-dose chest CT for lung cancer screening. Of these, 63 (12.6%) had a history of CHD, the remaining 438 subjects (87.4%) were clinically asymptomatic and without a history of CHD. On the day of the CT study, subjects underwent a thorough clinical examination including blood tests and completed a standardized questionnaire to establish a complete medical history. ECC and CAC scores were quantified according to Agatston and, in addition, by visual rating of calcium load of individual vessel territories on a five-point scale from “absent” to “extensive.” Results were correlated with the respective subjects’ cardiovascular risk factors and with the presence or absence of CHD.
Results
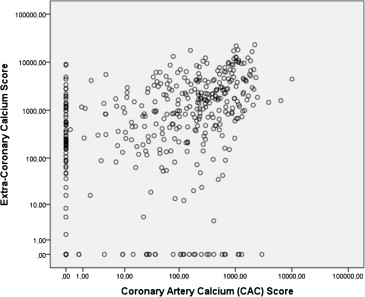
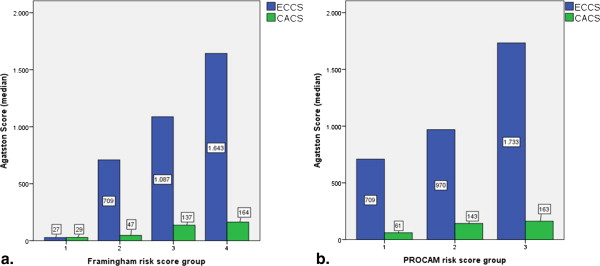
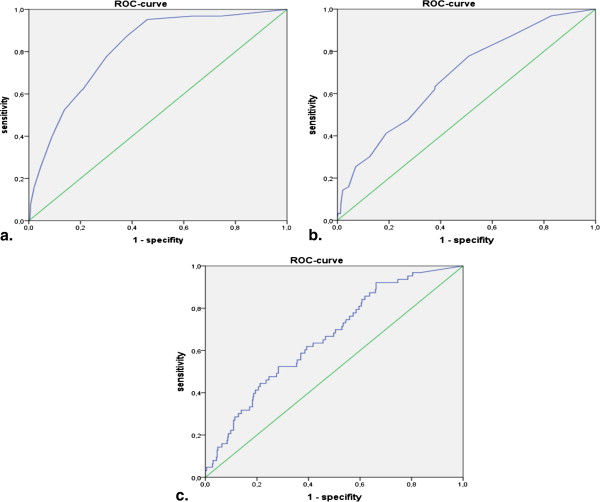
ECC scores correlated significantly with CAC scores (two-sided Spearman 0.515; P < .001). ECC scores were associated significantly ( P < .001) with cardiovascular risk factors (smoking history, hypertension, diabetes, and hypercholesterolemia) and with subjects’ Framingham/prospective cardiovascular münster study scores, whereas CAC scores were associated only with the presence of hypercholesterolemia. CAC scores were strongly associated with CHD than ECC scores (area under the curve, 0.88 vs. 0.66 at receiver operating characteristic analysis). Visual scoring of ECC/CAC load correlated closely with the respective Agatston values ( P < .001) and revealed the same association (or lack thereof) with cardiovascular risk factors/CHD.
Conclusions
In nongated low-dose CT for lung cancer screening, CAC and ECC load can be accurately established by visual analysis. ECC and CAC scores correlate closely, but not perfectly. There is a strong association between established cardiovascular risk factors and ECC load, but not CAC load, providing further evidence that ECC scoring may complement CAC scoring for broader risk assessment, for example, regarding prediction of extracoronary vascular events.
It is well established that coronary artery calcifications (CACs) as detected by multidetector computed tomography (MDCT) can be used to predict coronary heart disease (CHD) and future coronary events . Over the past decade, there has been accumulating evidence that extracoronary thoracic calcifications such as calcifications of the aortic valve , thoracic aorta, and mitral valve/annulus also seem to correlate with coronary calcified plaque burden , CHD , all-cause, and cardiovascular mortality .
Notwithstanding the observed correlation between coronary and extracoronary calcification (ECC), there is initial evidence that the predictive implications of calcifications for the different vascular territories do vary. ECCs, specifically aortic valve calcifications, have been shown to be a more powerful predictor of extracardiac vascular events such as ischemic stroke . It has also been shown that thoracic aortic calcifications are a significant predictor of future coronary events in women, independent of the degree of coronary calcifications .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and methods
Study Design and Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CHD and Cardiovascular Risk Factors
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MDCT Imaging Protocol
Get Radiology Tree app to read full this article<
Determining CAC and ECC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Study Cohort
Get Radiology Tree app to read full this article<
Table 1
Demographics and Medical History of the Study Cohort ( n = 501)
Demographics—all subjects ( n = 501) Mean SD Median No. of Subjects (%) Age, y 66.7 8.1 68.0 Body mass index, kg/m 2 29.8 14.3 28.9 Cardiovascular risk in subjects without diagnosis of CHD ( n = 438) Smoking history/pack-years Current smoker 24.2 18.3 22 317 72.4 Nonsmoker — — — 121 27.6 Hypertension 287 65.5 Diabetes type II 85 19.4 Hypercholesterolemia 280 63.9 Family history First-degree family history of premature CHD 101 23.1 Medication Lipid-lowering medication 96 21.9 Antihypertensive medication 242 55.3 Oral antidiabetics and/or insulin 66 15.1 Platelet aggregation inhibitor 81 18.5 Serologic markers Total cholesterol, mg/dL 216.8 37.6 216 373 HDL cholesterol level, mg/dL 52.3 14.3 49 245 LDL cholesterol level, mg/dL 136.5 36.3 135 240 Blood pressure Systolic blood pressure, mm Hg 139 18.4 140 373 Diastolic blood pressure, mm Hg 81.2 9.9 80 373 Patients with diagnosis of CHD ( n = 63) History of cardiac events History of myocardial infarction 23 36.5 History of cardiac catheterization 52 82.5 History of coronary stenting 32 50.7 History of CABG 52 82.5
CABG, coronary artery bypass surgery; CHD, coronary heart disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Get Radiology Tree app to read full this article<
Extracoronary and CACs
Get Radiology Tree app to read full this article<
Quantitative CAC and ECC Scoring in 438 Clinically Asymptomatic Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Quantitative ECC Scores by CAC Score Subgroups According to Rumberger in Asymptomatic Subjects ( n = 438)
CAC Score ECC Score No. of Subjects Median Percentile 25 Percentile 75 Mean Standard Deviation_P_ Value (Kruskal-Wallis Test) 0 113 153 0 509 605 1406 <.001 1–10 22 336 88 1126 934 1385 11–100 85 518 141 2062 1467 2179 101–400 92 1269 311 2319 2177 2945 >400 126 2201 677 5511 3928 4619
CAC, coronary artery calcification; ECC, extracoronary calcification.
Get Radiology Tree app to read full this article<
Visual CAC and ECC Scoring in the Entire Cohort (501 Subjects with and Without CHD)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation Between Visual and Quantitative CAC and ECC Scoring
Get Radiology Tree app to read full this article<
Correlation of ECC with CAC in 438 Clinically Asymptomatic Subjects
Correlation of Quantitative Scores
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation of Calcium Prevalence
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Association of ECC/CAC with Cardiovascular Risk Factors in 438 Clinically Asymptomatic Subjects
Quantitative CAC and ECC Scores Versus Risk Factors
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Association of ECC and CAC Scores with Cardiovascular Risk Factors in Asymptomatic Subjects ( n = 438)
CHD-Risk Factors Number of Subjects ECC Score CAC Score Median Mean_P_ Value Median Mean_P_ Value Smoking history No 121 494 1657 .002 74 306 .25 Yes 317 914 2236 99 385 Hypertension No 151 343 1188 .0001 45 284 .116 Yes 287 1089 2542 134 404 Diabetes No 353 677 1918 .023 76 354 .634 Yes 85 1145 2728 176 398 Hypercholesterolemia No 158 448 1912 .003 59 244 .013 Yes 280 973 2166 131 429 Family history No 337 825 2119 .571 79 348 .475 Yes 101 750 1928 129 410
CAC, coronary artery calcification; ECC, extracoronary calcifications.
Get Radiology Tree app to read full this article<
Visual Scores of ECC and CAC Versus Risk Factors
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation with Framingham and PROCAM Scores in 438 Clinically Asymptomatic Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation of ECC/CAC in 63 Patients with Overt CHD
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
2. Jacobs P.C., Gondrie M.J., van der Graaf Y., et. al.: Coronary artery calcium can predict all-cause mortality and cardiovascular events on low-dose CT screening for lung cancer. AJR Am J Roentgenol 2012; 198: pp. 505-511.
3. Pletcher M.J., Tice J.A., Pignone M., et. al.: Using the coronary artery calcium score to predict coronary heart disease events: a systematic review and meta-analysis. Arch Intern Med 2004; 164: pp. 1285-1292.
4. Youssef G., Budoff M.J.: Coronary artery calcium scoring, what is answered and what questions remain. Cardiovasc Diagn Ther 2012; 2: pp. 94-105.
5. Budoff M.J., Gul K.M.: Expert review on coronary calcium. Vasc Health Risk Manag 2008; 4: pp. 315-324.
6. Sverzellati N., Cademartiri F., Bravi F., et. al.: Relationship and prognostic value of modified coronary artery calcium score, FEV1, and emphysema in lung cancer screening population: the MILD trial. Radiology 2012; 262: pp. 460-467.
7. Rossi A., Gaibazzi N., Dandale R., et. al.: Aortic valve sclerosis as a marker of coronary artery atherosclerosis; a multicenter study of a large population with a low prevalence of coronary artery disease. Int J Cardiol 2014; 172: pp. 364-367.
8. Adler Y., Shemesh J., Tenenbaum A., et. al.: Aortic valve calcium on spiral computed tomography (dual slice mode) is associated with advanced coronary calcium in hypertensive patients. Coron Artery Dis 2002; 13: pp. 209-213.
9. Ann S.H., Jung J.I., Jung H.O., et. al.: Aortic valve calcium score is associated with coronary calcified plaque burden. Int Heart J 2013; 54: pp. 355-361.
10. Koos R., Kühl H.P., Mühlenbruch G., et. al.: Prevalence and clinical importance of aortic valve calcification detected incidentally on CT scans: comparison with echocardiography. Radiology 2006; 241: pp. 76-82.
11. Utsunomiya H., Yamamoto H.: Combined presence of aortic valve calcification and mitral annular calcification as a marker of the extent and vulnerable characteristics of coronary artery plaque assessed by 64-multidetector computed tomography. Atherosclerosis 2010; 213: pp. 166-172.
12. Yamamoto H., Shavelle D., Takasu J., et. al.: Valvular and thoracic aortic calcium as a marker of the extent and severity of angiographic coronary artery disease. Am Heart J 2003; 146: pp. 153-159.
13. Völzke H., Haring R., Lorbeer R., et. al.: Heart valve sclerosis predicts all-cause and cardiovascular mortality. Atherosclerosis 2010; 209: pp. 606-610.
14. Fox C.S., Vasan R.S., Parise H., et. al.: Framingham Heart Study. Mitral annular calcification predicts cardiovascular morbidity and mortality: the Framingham Heart Study. Circulation 2003; 197: pp. 1492-1496.
15. Owens D.S., Budoff M.J., Katz R., et. al.: Aortic valve calcium independently predicts coronary and cardiovascular events in a primary prevention population. JACC Cardiovasc Imaging 2012; 5: pp. 619-625.
16. Kälsch H., Lehmann N., Mahabadi A.A., et. al., Recall, on behalf of the Investigator Group of the Heinz Nixdorf: Beyond Framingham risk factors and coronary calcification: does aortic valve calcification improve risk prediction? The Heinz Nixdorf Recall Study. Heart 2014; 100: pp. 930-937.
17. Kizer J.R., Wiebers D.O., Whisnant J.P., et. al.: Mitral annular calcification, aortic valve sclerosis, and incident stroke in adults free of clinical cardiovascular disease: the Strong Heart Study. Stroke 2005; 36: pp. 2533-2537.
18. Jacobs P.C., Prokop M., van der Graaf Y., et. al.: Comparing coronary artery calcium and thoracic aorta calcium for prediction of all-cause mortality and cardiovascular events on low-dose non-gated computed tomography in a high-risk population of heavy smokers. Atherosclerosis 2010; 209: pp. 455-462.
19. Wong N.D., Lopez V.A., Allison M., et. al.: Abdominal aortic calcium and multi-site atherosclerosis: the multiethnic study of atherosclerosis (MESA). Atherosclerosis 2011; 214: pp. 436-441.
20. Budoff M.J., Nasir K., Katz R., et. al.: Thoracic aortic calcification and coronary heart disease events: the multi-ethnic study of atherosclerosis (MESA). Atherosclerosis 2011; 215: pp. 196-202.
21. The National Lung Screening Trial Research Team: Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365: pp. 395-409.
22. Kanne J.P.: Screening for lung cancer: what have we learned?. AJR Am J Roentgenol 2014; 202: pp. 530-535.
23. Marshall H.M., Bowman R.V., Yang I.A., et. al.: Screening for lung cancer with low-dose computed tomography: a review of current status. J Thorac Dis 2013; 5: pp. 524-539.
24. Jacobson F.L., Jaklitsch M.T.: Low-dose CT screening for lung cancer: the time is now. J Surg Oncol 2013; 108: pp. 265-269.
25. New York Early Lung Cancer Action Project Investigators: CT Screening for lung cancer: diagnoses resulting from the New York Early Lung Cancer Action Project. Radiology 2007; 243: pp. 239-249.
26. Horeweg N., van der Aalst C.M., Vliegenthart R., et. al.: Volumetric computed tomography screening for lung cancer: three rounds of the NELSON trial. Eur Respir J 2013; 42: pp. 1659-1667.
27. Arcadi T., Maffei E., Sverzellati N., et. al.: Coronary artery calcium score on low-dose computed tomography for lung cancer screening. World J Radiol 2014; 6: pp. 381-387.
28. Xie X., Greuter M.J., Groen J.M., et. al.: Can nontriggered thoracic CT be used for coronary artery calcium scoring? A phantom study. Med Phys 2013; 40: pp. 081915.
29. Mets O.M., Vliegenthart R., Gondrie M.J., et. al.: Lung cancer screening CT-based prediction of cardiovascular events. JACC Cardiovasc Imaging 2013; 6: pp. 899-907.
30. Grundy S.M., Cleeman J.I., Merz C.N., et. al.: Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004; 110: pp. 227-239.
31. Assmann G., Oberwittler W., Schulte H., et. al.: Prädiktion und Früherkennung der koronaren Herzkrankheit. Prospektive epidemiologische Studie bei Betriebsangehörigen im Raum Westfalen. Internist (Berl) 1980; 21: pp. 446-459.
32. Goff D.C., Lloyd-Jones D.M., Bennett G., et. al.: 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63: pp. 2935-2959.
33. Rumberger J.A., Brundage B.H., Rader D.J., et. al.: Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc 1999; 74: pp. 243-252.
34. Taylor A.J., Cerqueira M., Hodgson J., et. al.: ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 2010; 56: pp. 1864-1894.
35. National Lung Screening Trial Research Team, Church T.R., Black W.C., Aberle D.R., et. al.: Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med 2013; 368: pp. 1980-1991.
36. Greenland P., LaBree L., Azen S.P., et. al.: Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004; 291: pp. 210-215.
37. Hecht H.S., Budoff M.J., Berman D.S., et. al.: Coronary artery calcium scanning: clinical paradigms for cardiac risk assessment and treatment. Am Heart J 2006; 151: pp. 1139-1146.
38. Hecht H.S.: Subclinical atherosclerosis imaging comes of age: coronary artery calcium in primary prevention. Curr Opin Cardiol 2012; 27: pp. 508-514.
39. Allison M.A., Cheung P., Criqui M.H., et. al.: Mitral and aortic annular calcification are highly associated with systemic calcified atherosclerosis. Circulation 2006; 113: pp. 861-866.
40. Mahabadi A.A., Bamberg F., Toepker M., et. al.: Association of aortic valve calcification to the presence, extent, and composition of coronary artery plaque burden: from the Rule Out Myocardial Infarction using Computer Assisted Tomography (ROMICAT) trial. Am Heart J 2009; 158: pp. 562-568.
41. Kanjanauthai S., Nasir K., Katz R., et. al.: Relationships of mitral annular calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2010; 213: pp. 558-562.
42. Farrag A., Bakhoum S., Salem M.A., et. al.: The association between extracoronary calcification and coronary artery disease in patients with type 2 diabetes mellitus. Heart Vessels 2013; 28: pp. 12-18.
43. Gondrie M.J., van der Graaf Y., Jacobs P.C., et. al., PROVIDI Study Group: The association of incidentally detected heart valve calcification with future cardiovascular events. Eur Radiol 2011; 21: pp. 963-973.
44. Allison M.A., Pavlinac P., Wright C.M.: The differential associations between HDL, non-HDL and total cholesterols and atherosclerotic calcium deposits in multiple vascular beds. Atherosclerosis 2007; 194: pp. e87-e94. Epub 2006 Nov 16
45. Pletcher M.J., Sibley C.T., Pignone M., et. al.: Interpretation of the coronary artery calcium score in combination with conventional cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2013; 128: pp. 1076-1084.
46. Tison G.H., Blaha M.J., Budoff M.J., et. al.: The relationship of insulin resistance and extracoronary calcification in the multi-ethnic study of atherosclerosis. Atherosclerosis 2011; 218: pp. 507-510.
47. Shahzad R., van Walsum T., Schaap M., et. al.: Vessel specific coronary artery calcium scoring: an automatic system. Acad Radiol 2013; 20: pp. 1-9.
48. Isgum I., Prokop M., Niemeijer M., et. al.: Automatic coronary calcium scoring in low-dose chest computed tomography. IEEE Trans Med Imaging 2012; 31: pp. 2322-2334.