
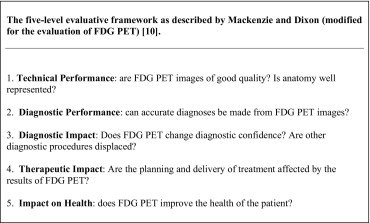
In today’s environment of progressively evolving and expensive imaging modalities, radiologists are asked to justify the use of resources to patients, referring physicians, hospital management, and third party payers. With this aim, the radiologist may use “top-down” or “bottom-up” “evidence-based practice” (EBP) techniques. “Top-down” suggests that the practitioner should wait until a higher authority, external to their practice, generates a solution to practice dilemmas (e.g., National Institute for Health and Clinical Excellence [NICE] guidelines). “Bottom-up” however, is based on the theory that the ordinary practitioner is best served by a decentralized approach to problem solving that is internal to their practice. The technology assessment framework modeled by Mackenzie and Dixon comprehensively assesses the effects of imaging using levels of efficacy including diagnostic performance, diagnostic impact, and therapeutic impact, impact on health and cost effectiveness. In this article, we describe how issues regarding new imaging modalities in ordinary radiology practice can be addressed by using stepwise “bottom-up” EBP techniques combined with the technology assessment framework. We also detail how EBP techniques form an integral part of practice-based learning among radiology residents as part of noninterpretive residency training. The following clinical scenario is used: Your hospital’s chief hepatobiliary surgeon writes to your department regarding the lack of access to 18-fluoro-2-deoxy- d -glucose positron emission tomography in the preoperative assessment of patients with colorectal cancer liver metastases under consideration for hepatic resection. How would you approach this problem? Here is how we would do it.
Clinical scenario
You are an attending radiologist in a busy hepatobiliary tertiary referral centre. The hepatobiliary surgical chairman writes a letter to you concerning the lack of availability of 18-fluoro-2-deoxy- d -glucose positron emission tomography (FDG PET) in the preoperative assessment of patients with colorectal cancer liver metastases (CRCLMs) who are under consideration for hepatic resection. The letter reads as follows:
As you know, the liver is the most frequent site for colorectal cancer metastasis with half of all patients with colorectal cancer developing liver metastases ( ). More than 20% of patients with colorectal cancer have liver metastases at the time of diagnosis, while 40−60% of relapsed patients have CRCLMs ( ). Hepatic resection of CRCLMs is the accepted standard of care and one of the few curative options available to patients.
Accurate preoperative staging is essential in the management of CRCLMs to prevent unnecessary laparotomy in patients who are found to be unresectable at surgery and correctly select those patients with potential for curative resection. FDG PET is a rapidly emerging clinical application in the detection of hepatic and extrahepatic colorectal metastases. Despite this, FDG PET is not available to all our patients being assessed for hepatic resection. It would appear the limited availability and the high cost of FDG PET are restricting its use. I note also in my own research regarding the imaging modality that there is very limited cost-effectiveness data on FDG PET.
I have found on a number of occasions that computed tomography (CT) and magnetic resonance imaging (MRI) have understaged patients on whom I have attempted hepatic resection. This has led to unnecessary surgery, morbidity, and cost. In the environment in which we work where there are limited resources with respect to intensive care unit beds and operating theater time, this is putting a strain on an overburdened service. I believe that FDG PET will stage this patient subgroup more accurately, will impact their management, and may prove to be cost effective.
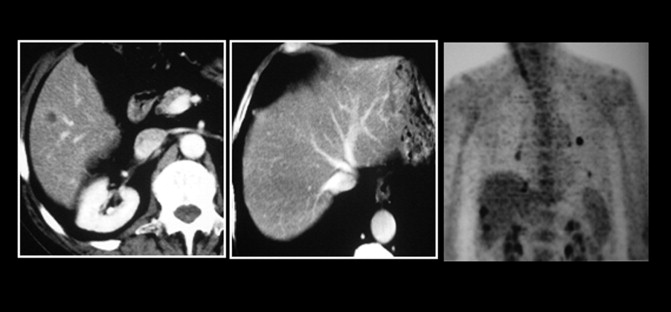
Recently you used EBP techniques to justify the use of transarterial chemoembolization in the management of hepatocellular carcinoma ( ) ( Fig. 1 ). I would appreciate if you could again use EBP techniques to evaluate the role of FDG PET in the management of patients with CRCLMs.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
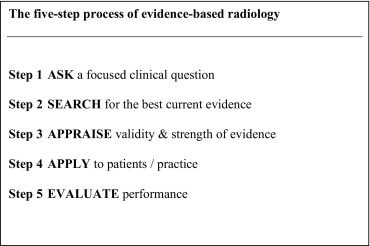
Evidence-based practice: The stepwise process
Get Radiology Tree app to read full this article<
Step 1: Ask
Get Radiology Tree app to read full this article<
Step 2: Search
Get Radiology Tree app to read full this article<
Step 3: Appraise
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Studies Analyzing the Diagnostic and Therapeutic Impact of FDG PET
Study ⁎ Sample Size Diagnostic Impact Major Management Impact Simo et al [ ] 120 — 48% Kalff et al [ ] 102 — 59% Meta et al [ ] 60 42% 37% Imdahl et al [ ] 71 — 20%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Step 4: Apply
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Step 5: Evaluate the change in practice
Get Radiology Tree app to read full this article<
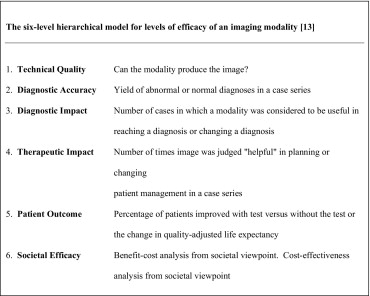
Technology assessment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diagnostic impact
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Therapeutic impact
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
The Five-Step EBP Process Can Be Used to Devise Department Protocols
Get Radiology Tree app to read full this article<
The Technology Assessment Framework Is Useful in Assessing FDG PET
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG PET Has a Diagnostic Impact
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG PET Has a Therapeutic Impact
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG PET Is Effective
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Arulampalam T.H., Francis D.L., Visvikis D., Taylor I.J., Ell P.: FDG-PET for the pre-operative evaluation of colorectal liver metastases. Eur J Surg Oncol 2004; 30: pp. 286-291.
2. Fiorentini G., Poddie D.B., De Giorgi U., et. al.: Global approach to hepatic metastases from colorectal cancer: Indication and outcome of intra-arterial chemotherapy and other hepatic-directed treatments. Med Oncol 2000; 17: pp. 163-173.
3. Staunton M., Dodd J.D., McCormick P.A., Malone D.E.: Finding evidence-based answers to practical questions in radiology: Which patients with inoperable hepatocellular carcinoma will survive longer after transarterial chemoembolization?. Radiology 2005; 237: pp. 404-413.
4. Maher M.M., McNamara M.M., McEneaney P.M., Sheehan S.J., Malone D.E.: Abdominal aortic aneurysms: Elective endovascular repair versus conventional surgery-evaluation with evidence-based medicine techniques. Radiology 2003; 228: pp. 647-658.
5. Centre for Evidence Based Medicine, University of Oxford. Levels of evidence and grades of recommendations. Available at www.cebm.net/levels of evidence.asp . Accessed January 10, 2007. Available at www.cebm.net/levels of evidence.asp . Accessed January 10, 2007.
6. Kinkel K., Lu Y., Both M., Warren R.S., Thoeni R.F.: Detection of hepatic metastases from cancers of the gastrointestinal tract by using noninvasive imaging methods (US, CT, MR imaging, PET): A meta-analysis. Radiology 2002; 224: pp. 748-756.
7. Bipat S., van Leeuwen M.S., Comans E.F.I., Pijl M.E.J., Bossuyt P.M.M., Zwinderman A.H., Stoker J.: Colorectal liver metastases: CT, MR imaging, and PET for diagnosis-meta-analysis. Radiology 2005; 237: pp. 123-131.
8. Fineberg H.V., Bauman R., Sosman M.: Computerized cranial tomography. JAMA 1977; 238: pp. 224-227.
9. Rosenberg W., Donald A.: Evidence based medicine: An approach to clinical problem-solving. BMJ 1995; 310: pp. 1122-1126.
10. Mackenzie R., Dixon A.K.: Measuring the effects of imaging: An evaluative framework. Clin Radiol 1995; 50: pp. 513-518.
11. Leskinnen-Kallio S.: Positron emission tomography in oncology. Clin Physiol 1994; 14: pp. 329-335.
12. Collins J., de Christenson M.R., Gray L., et. al.: General competencies in radiology residency training: Definitions, skills, education and assessment. Acad Radiol 2002; 9: pp. 721-726.
13. Fryback D.G., Thornbury J.R.: The efficacy of diagnostic imaging. Med Decis Making 1991; 11: pp. 88-94.
14. Zubeldia J.M., Bednarczyk E.M., Baker J.G., Nabi H.A.: The economic impact of 18FDG positron emission tomography in the surgical management of colorectal cancer with hepatic metastases. Cancer Biother Radiopharm 2005; 20: pp. 450-456.
15. Fong Y., Saldinger P.F., Akhurst T., et. al.: Utility of 18F-FDG positron emission tomography scanning on selection of patients for resection of hepatic colorectal metastases. Am J Surg 1999; 178: pp. 282-287.
16. Bengmark S.: Palliative treatment of hepatic tumours. Br J Surg 1989; 76: pp. 771-773.
17. Steele G., Bleday R., Mayer R.J., Lindblad A., Petrelli N., Weaver D.: A prospective evaluation of hepatic resection for colorectal carcinoma metastases to the liver: Gastrointestinal Tumor Study Group Protocol 6584. J Clin Oncol 1991; 9: pp. 1105-1112.
18. Elias D., Sideris L., Pocard M., et. al.: Incidence of unsuspected and treatable metastatic disease associated with operable colorectal liver metastases discovered only at laparotomy (and not treated when performing percutaneous radiofrequency ablation). Ann Surg Oncol 2005; 12: pp. 298-302.
19. Simo M., Lomena F., Setoain J., et. al.: FDG-PET improves the management of patients with suspected recurrence of colorectal cancer. Nucl Med Commun 2002; 23: pp. 975-982.
20. Truant S., Huglo D., Hebbar M., Ernst O., Steinling M., Pruvot F.R.: Prospective evaluation of the impact of [18F] fluoro-2-deoxy-D-glucose positron emission tomography of resectable colorectal liver metastases. Br J Surg 2005; 92: pp. 362-369.
21. Teague B.D., Morrison C.P., Court F.G., et. al.: Role of FDG-PET in surgical management of patients with colorectal liver metastases. ANZ J Surg 2004; 74: pp. 646-652.
22. Fernandez F.G., Drebin J.A., Linehan D.C., Dehdashti F., Siegel B.A., Strasberg S.M.: Five-year survival after resection of hepatic metastases from colorectal cancer in patients screened by positron emission tomography with F-18 fluorodeoxyglucose (FDG-PET). Ann Surg 2004; 240: pp. 438-447.
23. Brook R.H., Lohr K.N.: Efficacy, effectiveness, variations, and quality. Med Care 1985; 23: pp. 710-722.
24. Kalff V., Hicks R.J., Ware R.E., Hogg A., Binns D., McKenzie A.F.: The clinical impact of (18) F-FDG PET in patients with suspected or confirmed recurrence of colorectal cancer: A prospective study. J Nucl Med 2002; 43: pp. 492-499.
25. Meta J., Seltzer M., Schiepers C., et. al.: Impact of 18 F-FDG PET on managing patients with colorectal cancer: The referring physician’s perspective. J Nucl Med 2001; 42: pp. 586-590.
26. Imdahl A., Reinhardt M.J., Nitzsche E.U., et. al.: Impact of 18F-FDG-positron emission tomography for decision making in colorectal cancer recurrences. Langenbecks Arch Surg 2000; 385: pp. 129-134.