
The proceedings of a workshop focusing on a project to evaluate the use of fluorodeoxyglucose-positron emission tomography (FDG-PET) as a tool to measure treatment response in non-Hodgkin lymphoma (NHL) are described. Sponsored by the Leukemia & Lymphoma Society, the Foundation of the National Institutes of Health, and the National Cancer Institute, and attended by representatives of the Food and Drug Administration, the Centers for Medicare and Medicaid Services, and scientists and clinical researchers from academia and the pharmaceutical and medical imaging industries, the workshop reviewed the etiology and current standards of care for NHL and proposed the development of a clinical trial to validate FDG-PET imaging techniques as a predictive biomarker for cancer therapy response. As organized under the auspices of the Oncology Biomarker Qualification Initiative, the three federal health agencies and their private sector and nonprofit/advocacy group partners believe that FDG-PET not only demonstrates the potential to be used for the diagnosis and staging of many cancers but in particular can provide an early indication of therapeutic response that is well correlated with clinical outcomes for chemotherapy for this common form of lymphoma. The development of standardized criteria for FDG-PET imaging and establishment of procedures for transmission, storage, quality assurance, and analysis of PET images afforded by this demonstration project could streamline clinical trials of new treatments for more intractable forms of lymphoma and other cancers and, hence, accelerate new drug approvals.
As David Timko spoke to this gathering of clinical oncologists and imaging scientists, he reflected on the irony of learning that he had non-Hodgkin lymphoma (NHL) after years of service to the Leukemia & Lymphoma Society (L&LS): “I was devastated by the diagnosis in 1993, and knew my treatment would be challenging,” but he also knew that the odds of curing the disease had improved markedly in recent years. He reflected on three important research advances: development of the hematopoietic growth factor Neupogen, improved antiemetic agents, and markedly more sensitive diagnostic tools. These helped him avoid infection, retain his weight, and tolerate higher curative doses of chemotherapy and showed that he was free of disease and unlikely to have to endure a potentially more dangerous bone marrow transplant (a standard follow-on treatment for many patients before the adoption of molecular diagnostic methods). Now in remission for more than 10 years, he remarked that these advances in biomedicine and technology reached the marketplace and were incorporated into clinical practice in time to benefit individuals like himself, but that there are others who still are not cured. He charged those in the audience to focus on how to move potentially even more significant new drugs and technologies through the development and regulatory approval process, “Every advance is another life saved.”
The meeting he was addressing, The FDG-PET Lymphoma Demonstration Project Workshop, was held at the William H. Natcher Building on the National Institutes of Health (NIH) campus on March 20, 2006, and was sponsored jointly by The Foundation of the NIH (FNIH) and L&LS. Addressing Timko’s plea, the primary objective of this workshop was a clinical development plan for technology to advance the treatment of lymphoma, i.e., 18 F-fluorodeoxyglucose positron emission tomography (FDG-PET), to measure response to chemotherapy for lymphoma. This plan will be carried out under the Oncology Biomarker Qualification Initiative (OBQI).
The OBQI, announced in February 2006, is an agreement among the National Cancer Institute (NCI), United States Food and Drug Administration (FDA), and Centers for Medicare and Medicaid Services (CMS) to collaborate on improving the development of cancer therapies and the outcomes for cancer patients through biomarker development and evaluation. The goal of OBQI is to validate particular biomarkers so that they can be used to evaluate new, promising technologies in a manner that will shorten clinical trials, reduce the time and resources spent during the drug development process, improve the linkage between drug approval and drug coverage, and increase the safety and appropriateness of drug choices for cancer patients. Under the OBQI, biomarker research will focus on four key areas: standardizing and evaluating imaging technologies to allow better visualization of how cancer therapies are working; developing scientific bases for diagnostic assays to enable personalized treatments; instituting new trial designs to utilize biomarkers, and pooling data to ensure that key lessons are shared from one trial to another. By working with academic and industry scientists, as well as professional organizations, the OBQI teams will foster the development of key information on biomarkers through clinical trials.
Why FDG-PET? Why lymphoma?
In oncology, the gold standard clinical trial endpoint is overall survival (OS), which may require long-term studies and may be confounded by deaths from causes other than the patient’s cancer. Over the years, the oncology community and the FDA in evaluating oncologic therapies have come to rely on other endpoints that from a scientific perspective are regarded as correlates of clinical benefit. These endpoints are objective response (OR), time to progression (TTP), disease-free survival (DFS), and progression-free survival (PFS). All are determined by biomarkers measuring the cancer’s extent. Anatomic imaging using one- or two-dimensional measurements to characterize cancers has been used traditionally to make these measurements in all aspects of cancer patient management from diagnosis and staging to monitoring response to therapy and disease progression.
However, measurements made using standard anatomic imaging techniques are often inadequate for characterizing the cancer, especially for monitoring the effects of drugs that do not cause tumor shrinkage or for cancers that progress slowly or metastasize diffusely. Newer imaging modalities including FDG-PET show high promise as the basis for characterizing better biomarkers of cancer [see Table 1 , reviewed in ( )]. Further, some forms of lymphoma, including Hodgkin disease (HD), and diffuse large B-cell NHL (DLBCL), provide good clinical settings for the evaluation of FDG-PET−based biomarkers because they can be managed successfully with known effective drugs, because FDG-PET data already exist for diagnosis and staging (FDG-PET has been reimbursed by CMS for these purposes since 1999), and because response criteria have been established that can be refined using FDG-PET ( ). In these diseases, FDG-PET has the potential to improve patient management, particularly by signaling the need for early therapeutic changes in nonresponders (NR) ( ) and by refining the International Working Group (IWG) response criteria to better differentiate complete responses (CR), partial responses (PR), and complete response with residual mass (CRu, unconfirmed due to residual tumor mass) ( ). Thus, if the utility of FDG-PET as a biomarker can be confirmed in such settings ( Table 2 ), unnecessary chemotherapy may be avoided for some patients and the costs of unnecessary long-term follow-up reduced. As an early surrogate endpoint for clinical benefit, FDG-PET also has the potential to facilitate the development of new drug treatments by shortening Phase 2 trials and detecting clinical benefit earlier in Phase 3 investigations.
Table 1
Basis for Pursuing the Validation of FDG-PET as a Biomarker of Response to Cancer Treatment
Get Radiology Tree app to read full this article<
See Kelloff et al. ( ).
Table 2
Why FDG-PET–Derived Biomarkers Will be Useful in Lymphoma
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
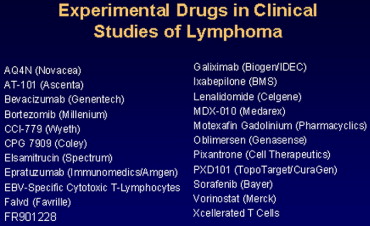
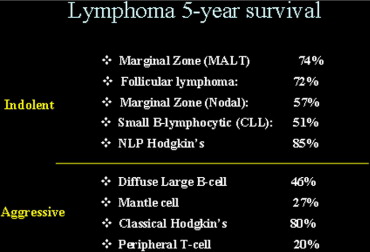
Pathobiology and therapy of lymphoma
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
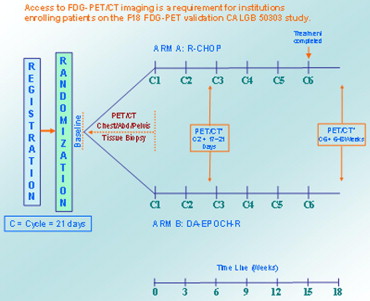
DLBCL as clinical cohort for assessment of FED-PET endpoints
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG-PET measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical considerations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Requirements for validation of FDG-PET−based biomarkers from a regulatory perspective
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG-PET in phase 2 studies of novel drugs
Get Radiology Tree app to read full this article<
Characteristics of FDG-PET images in lymphoma
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quality assurance of FDG-PET data
Get Radiology Tree app to read full this article<
Discussion and conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kelloff G.J., Hoffman J.M., Johnson B., et. al.: Progress and promise of FDG-PET imaging for cancer patient management and oncologic drug development. Clin Cancer Res 2005; 11: pp. 2785-2808.
2. Cheson B.D., Horning S.J., Coiffier B., et. al., NCI Sponsored International Working Group: Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. J Clin Oncol 1999; 17: pp. 1244.
3. Juweid M.E., Wiseman G.A., Vose J.M., et. al.: Response assessment of aggressive non-Hodgkin’s lymphoma by integrated International Workshop Criteria and fluorine-18-fluorodeoxyglucose positron emission tomography. J Clin Oncol 2005; 23: pp. 4652-4661.
4. Haioun C., Itti E., Rahmouni A., et. al.: [18F]Fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) in aggressive lymphoma: An early prognostic tool for predicting patient outcome. Blood 2005; 106: pp. 1376-1381.
5. Meignan M., Haioun C., Itti E., Rahmouni A., Reyes F.: Value of [18F]fluorodeoxyglucose-positron emission tomography in managing patients with aggressive non-Hodgkin’s lymphoma. Clin Lymphoma Myeloma 2006; 6: pp. 306-313.
6. Hutchings M., Loft A., Hansen M., et. al.: FDG-PET after two cycles of chemotherapy predicts treatment failure and progression-free survival in Hodgkin lymphoma. Blood 2006; 107: pp. 52-59.
7. Spaepen K., Stroobants S., Dupont P., et. al.: Prognostic value of positron emission tomography (PET) with fluorine-18 fluorodeoxyglucose ([18F]FDG) after first-line chemotherapy in non-Hodgkin’s lymphoma: Is [18F]FDG-PET a valid alternative to conventional diagnostic methods?. J Clin Oncol 2001; 19: pp. 414-419.
8. Juweid M.E., Cheson B.D.: Role of positron emission tomography in lymphoma. J Clin Oncol 2005; 23: pp. 4577-4580.
9. Juweid M.E., Cheson B.D.: Positron-emission tomography and assessment of cancer therapy. N Engl J Med 2006; 354: pp. 496-507.
10. Shankar L.K., Hoffman J.M., Bacharach S., et. al.: Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute trials. J Nucl Med 2006; 47: pp. 1059-1066.
11. Armitage J.O.: Staging non-Hodgkin lymphoma. CA Cancer J Clin 2005; 55: pp. 368-376.
12. Shipp M.A.: Can we improve upon the International Index?. Ann Oncol 1997; 8: pp. 43-47.
13. Spaepen K., Stroobants S., Dupont P., et. al.: Early restaging positron emission tomography with (18)F-fluorodeoxyglucose predicts outcome in patients with aggressive non-Hodgkin’s lymphoma. Ann Oncol 2002; 13: pp. 1356-1363.
14. Kostakoglu L., Coleman M., Leonard J.P., Kuji I., Zoe H., Goldsmith S.J.: PET predicts prognosis after 1 cycle of chemotherapy in aggressive lymphoma and Hodgkin’s disease. J Nucl Med 2002; 43: pp. 1018-1027.
15. Freedman N.M., Sundaram S.K., Kurdziel K., et. al.: Comparison of SUV and Patlak slope for monitoring of cancer therapy using serial PET scans. Eur J Nucl Med Mol Imaging 2003; 30: pp. 46-53.
16. Weber W.A., Ziegler S.I., Thodtmann R., Hanauske A.R., Schwaiger M.: Reproducibility of metabolic measurements in malignant tumors using FDG PET. J Nucl Med 1999; 40: pp. 1771-1777.
17. Engles J.M., Quarless S.A., Mambo E., Ishimori T., Cho S.Y., Wahl R.L.: Stunning and its effect on 3H-FDG uptake and key gene expression in breast cancer cells undergoing chemotherapy. J Nucl Med 2006; 47: pp. 603-608.
18. Mikhaeel N.G., Hutchings M., Fields P.A., O’Doherty M.J., Timothy A.R.: FDG-PET after two to three cycles of chemotherapy predicts progression-free and overall survival in high-grade non-Hodgkin lymphoma. Ann Oncol 2005; 16: pp. 1514-1523.
19. Jerusalem G., Beguin Y., Fassotte M.F., et. al.: Persistent tumor 18F-FDG uptake after a few cycles of polychemotherapy is predictive of treatment failure in non-Hodgkin’s lymphoma. Haematologica 2000; 85: pp. 613-618.
20. Friedberg J.W., Chengazi V.: PET scans in the staging of lymphoma: Current status. Oncologist 2003; 8: pp. 438-447.
21. Gallamini A., Rigacci L., Merli F., et. al.: The predictive value of positron emission tomography scanning performed after two courses of standard therapy on treatment outcome in advanced stage Hodgkin’s disease. Haematologica 2006; 91: pp. 475-481.
22. Larson S.M., Erdi Y., Akhurst T., et. al.: Tumor treatment response based on visual and quantitative changes in global tumor glycolysis using PET-FDG imaging. Clin Positron Imaging 1999; 2: pp. 159-171.