
Rationale and Objectives
This study aimed to develop and implement a respiratory-gated setup for dual-source computed tomography (CT) at high pitch to examine patients in a reproducible inspiratory phase.
Materials and Methods
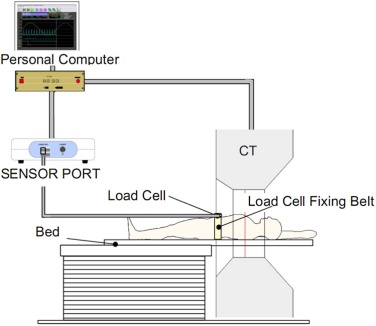
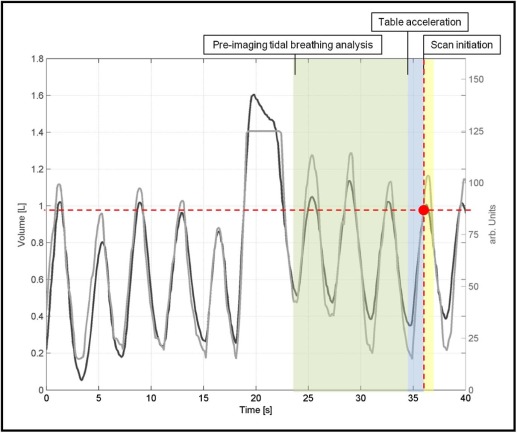
Twenty-one patients underwent free-breathing respiratory-gated chest CT using a high-pitch scan mode no more than 6 months after inspiratory breath-held nongated CT, which serves as reference. Scan parameters were as follows: pitch = 3.4, 128 × 0.6 mm collimation, 0.28 s gantry rotation time, and 150 ref.mAs per tube at 120 kV. The examinations were triggered using the tidal wave provided by a respiratory-gating system as input signal. Image quality was assessed focusing on artifacts and delineation of the anatomical and pathological structures. Lung volumes were measured on both free-breathing and reference examinations.
Results
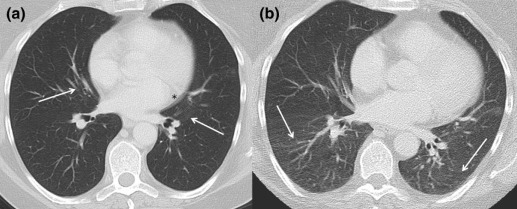
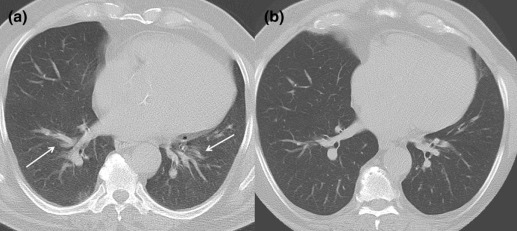
All examinations were performed without complications. Image quality was high with both protocols. Significantly less motion artifacts were recorded with the high-pitch mode compared to the reference ( P = 0.02). Most of the artifacts were located in the peripheral parts of the lower lobes for the study group and in the central part of the left lower lobe for the reference. Average total lung volume was 4.5 ± 1.5 L in respiratory-gated examinations and 5.8 ± 0.9 L in examinations with breath-hold in inspiration.
Conclusions
High-pitch chest CT scanning during free breathing minimizes motion artifacts, improving image quality in patients with limited breath-holding abilities. To assure scanning in an inspiratory phase, data acquisition should be triggered with a respiratory-gating system.
Introduction
Computed tomography (CT) has an important role to play in thoracic imaging . Isotropic imaging of the chest is possible with modern multislice spiral CT systems in less than 10 s, a breath-hold time that can be managed by the majority of patients. As a consequence of the shorter scan times, respiratory motion artifacts decreased and image quality improved significantly. Shorter CT rotation times also enabled higher temporal resolution and significantly reduced cardiac motion artifacts, which are not only known to alter the image quality near the heart, but also responsible for pulsation artifacts around the aorta and central pulmonary vessels .
However, there is a group of patients that cannot comply with breathing commands, for example ventilated patients, sedated patients, mentally impaired patients, or pediatric patients. Hence, image quality is commonly degraded from motion artifacts in these patient groups.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Population
Get Radiology Tree app to read full this article<
CT Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Control Group and Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Estimation of Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Conventional CT
Get Radiology Tree app to read full this article<
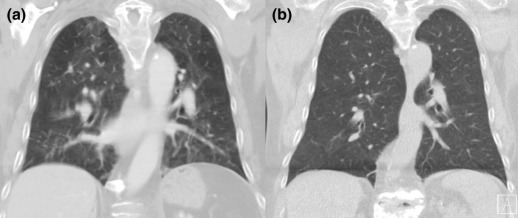
TABLE 1
Pathological Findings
Respiratory Gating Conventional Nodules 15 16 Consolidations 7 6 Masses 3 3 Interstitial lung disease 2 2 Ground glass opacities 7 9 Atelectasis 2 0
TABLE 2
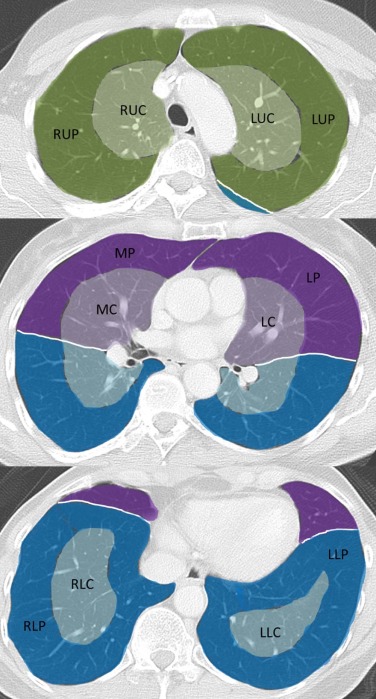
Rating of Motion Artifacts in the Defined Anatomical Regions
Conventional 1 2 3 4 Excellent Good Moderate Poor RUC 17 4 — — RUP 18 3 — — MC 15 3 3 — MP 17 2 2 — RLC 14 5 2 — RLP 19 1 1 — LUC 16 5 — — LUP 18 3 — — LC 13 6 2 — LP 17 3 1 — LLC 5 12 4 — LLP 17 3 1 —
Respiratory Gating 1 2 3 4 Excellent Good Moderate Poor RUC 19 2 — — RUP 14 6 1 — MC 21 — — — MP 17 4 — — RLC 19 2 — — RLP 12 9 — — LUC 20 1 — — LUP 14 6 1 — LC 20 1 — — LP 15 6 — — LLC 17 4 — — LLP 11 9 1 —
LC, lingula central; LP, lingula peripheral; LUC, left upper lobe central; LUP, left upper lobe peripheral; MC, middle lobe central; MP, middle lobe peripheral; RLC, left lower lobe central; RLC, right lower lobe central; RLP, left lower lobe peripheral; RLP, right lower lobe peripheral; RUC, right upper lobe central; RUP, right upper lobe peripheral.
Get Radiology Tree app to read full this article<
High-pitch CT
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Mohammed T.L., Chowdhry A., Reddy G.P., et. al.: ACR Appropriateness Criteria® screening for pulmonary metastases. J Thorac Imaging 2011; 26: pp. W1-W3.
2. Heitkamp D.E., Mohammed T.L., Kirsch J., et. al.: ACR appropriateness criteria(®)acute respiratory illness in immunocompromised patients. J Am Coll Radiol 2012; 9: pp. 164-169.
3. Lurz M., Lell M.M., Wuest W., et. al.: Automated tube voltage selection in thoracoabdominal computed tomography at high pitch using a third-generation dual-source scanner: image quality and radiation dose performance. Invest Radiol 2015; 50: pp. 352-360.
4. Petersilka M., Bruder H., Krauss B., et. al.: Technical principles of dual source CT. Eur J Radiol 2008; 68: pp. 362-368.
5. Achenbach S., Marwan M., Ropers D., et. al.: Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010; 31: pp. 340-346.
6. Lell M., Marwan M., Schepis T., et. al.: Prospectively ECG-triggered high-pitch spiral acquisition for coronary CT angiography using dual source CT: technique and initial experience. Eur Radiol 2009; 19: pp. 2576-2583.
7. Lell M., Hinkmann F., Anders K., et. al.: High-pitch electrocardiogram-triggered computed tomography of the chest: initial results. Invest Radiol 2009; 44: pp. 728-733.
8. Tacelli N., Remy-Jardin M., Flohr T., et. al.: Dual-source chest CT angiography with high temporal resolution and high pitch modes: evaluation of image quality in 140 patients. Eur Radiol 2010; 20: pp. 1188-1196.
9. Baumueller S., Alkadhi H., Stolzmann P., et. al.: Computed tomography of the lung in the high-pitch mode: is breath holding still required?. Invest Radiol 2011; 46: pp. 240-245.
10. Lell M.M., May M., Deak P., et. al.: High-pitch spiral computed tomography: effect on image quality and radiation dose in pediatric chest computed tomography. Invest Radiol 2011; 46: pp. 116-123.
11. Mortimer A.M., Singh R.K., Hughes J., et. al.: Use of expiratory CT pulmonary angiography to reduce inspiration and breath-hold associated artefact: contrast dynamics and implications for scan protocol. Clin Radiol 2011; 66: pp. 1159-1166.
12. Shrimpton P.C., Hillier M.C., Lewis M.A., et. al.: National survey of doses from CT in the UK: 2003. Br J Radiol 2006; 79: pp. 968-980.
13. Landis J.R., Koch G.G.: The measurement of observer agreement for categorical data. Biometrics 1977; 33: pp. 159-174.
14. Hausleiter J., Bischoff B., Hein F., et. al.: Feasibility of dual-source cardiac CT angiography with high-pitch scan protocols. J Cardiovasc Comput Tomogr 2009; 3: pp. 236-242.
15. Leschka S., Stolzmann P., Desbiolles L., et. al.: Diagnostic accuracy of high-pitch dual-source CT for the assessment of coronary stenoses: first experience. Eur Radiol 2009; 19: pp. 2896-2903.
16. Amacker N.A., Mader C., Alkadhi H., et. al.: Routine chest and abdominal high-pitch CT: an alternative low dose protocol with preserved image quality. Eur J Radiol 2012; 81: pp. e392-e397.
17. Achenbach S., Marwan M., Schepis T., et. al.: High-pitch spiral acquisition: a new scan mode for coronary CT angiography. J Cardiovasc Comput Tomogr 2009; 3: pp. 117-121.
18. Bischoff B., Meinel F.G., Del Prete A., et. al.: High-pitch coronary CT angiography in dual-source CT during free breathing vs. breath holding in patients with low heart rates. Eur J Radiol 2013; 82: pp. 2217-2221.