
Rationale and Objectives
The aim of this study was to investigate the clinical importance and height definition of flat (nonpolypoid) colorectal lesions detected on screening computed tomographic colonography (CTC).
Materials and Methods
Results from prospective screening CTC in 5107 consecutive asymptomatic adults (mean age, 56.9 years) at a single center were analyzed. All detected colorectal lesions ≥ 6 mm were prospectively categorized as polypoid or flat (nonpolypoid). The maximal height of all flat lesions was measured to assess the suggested 3-mm threshold definition.
Results
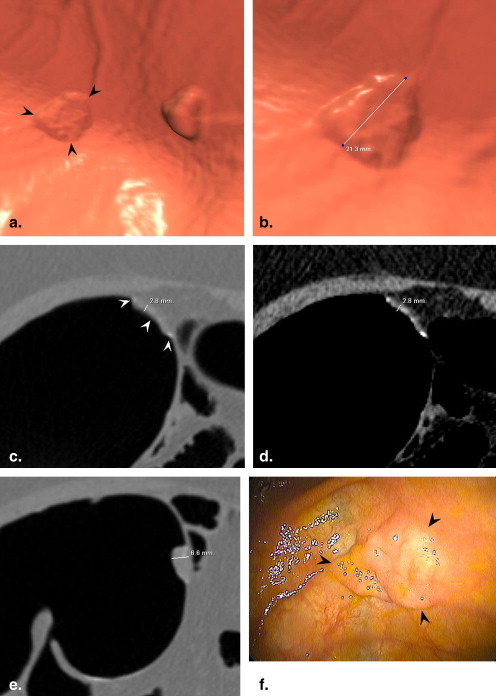
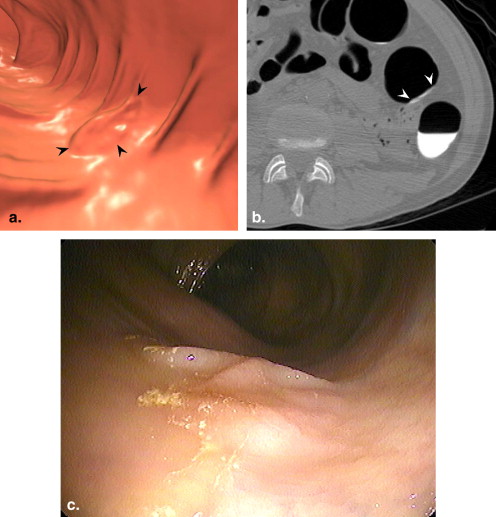
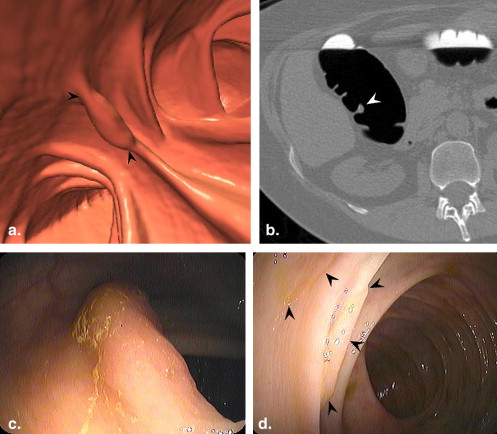
Of 954 polyps measuring ≥ 6 mm identified on screening CTC, 125 lesions (13.1%) in 106 adults were prospectively categorized as flat, with a mean size of 12.7 mm (range, 6–80 mm), including 73 lesions 6 to 9 mm, 42 lesions 10 to 29 mm, and 10 lesions ≥ 3 cm (carpet lesions). For polyps between 6 and 30 mm in size, flat lesions were less likely than polypoid lesions to be neoplastic (25.0% vs 60.3%, P < .001), histologically advanced (5.4% vs 12.1%, P = .07) or malignant (0% vs 0.5%, P = NS). Two of 10 carpet lesions (20%) were malignant, compared to 50% of polypoid masses ≥ 3 cm. Of nine flat lesions seen only on colonoscopy (false-negatives on CTC), two were neoplastic (tubular adenomas), and none was histologically advanced. For all flat lesions between 6 and 30 mm, the maximal height averaged 2.2 mm and was ≤3 mm in 86.1%, including 93.2% of small 6-mm to 9-mm flat lesions.
Conclusion
In a US screening population, flat colorectal lesions detected on CTC demonstrated less aggressive histologic features compared to polypoid lesions. Excluding carpet lesions, a maximal height of 3 mm appears to be a reasonable definition.
The true prevalence and potential clinical significance of “flat” or “nonpolypoid” colorectal lesions in the US screening population have been the source of recent debate . Some investigators have suggested that flat colorectal lesions may be more common and aggressive than previously thought. Unfortunately, a number of interrelated factors have combined to complicate the proper analysis of this issue, most notably the lack of standard definitions, but also potential geographic population differences (eg, East Asia vs the United States), mixing of high-risk and screening cohorts, varying detection strategies, and differences in histopathologic assessment. The term “flat” is actually somewhat of a misnomer, because truly flat lesions are extremely rare . Rather, this term generally describes lesions that are superficially elevated.
The issue of flat lesions is a potentially important consideration for computed tomographic (CT) colonography (CTC), particularly if this emerging test is to be used in population screening. As is the case with optical colonoscopy, flat lesions on CTC are generally less conspicuous than polypoid lesions of a similar size but may still detectable with appropriate technique and awareness.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Prevalence and Histologic Features of Polyps Detected on CTC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Morphologic Features of Flat (Nonpolypoid) Lesions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Flat Lesions Identified Only on Colonoscopy (False-negatives on CTC)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Soetikno R.M., Kaltenbach T., Rouse R.V., et. al.: Prevalence of nonpolypoid (flat and depressed) colorectal neoplasms in asymptomatic and symptomatic adults. JAMA 2008; 299: pp. 1027-1035.
2. Pickhardt P.J., Levin B., Bond J.H.: Screening for nonpolypoid colorectal neoplasms. JAMA 2008; 299: pp. 2743.
3. Robbins J, Pickhardt PJ, Kim DH. Flat (nonpolypoid) lesions detected at CT colonography. Presented at: Annual meeting of the Society of Gastrointestinal Radiologists; 2009.
4. Pickhardt P.J., Kim D.H.: Colorectal cancer screening with CT colonography: key concepts regarding polyp prevalence, size, histology, morphology, and natural history. AJR Am J Roentgenol 2009; 193: pp. 40-46.
5. Bond J.H.: Small flat adenomas appear to have little clinical importance in Western countries. Gastrointest Endosc 1995; 42: pp. 184-187.
6. Fidler J., Johnson C.: Flat polyps of the colon: accuracy of detection by CT colonography and histologic significance. Abdom Imaging 2009; 34: pp. 157-171.
7. O’Brien M.J., Winawer S.J., Zauber A.G., et. al.: Flat adenomas in the National Polyp Study: is there increased risk for high-grade dysplasia initially or during surveillance?. Clin Gastroenterol Hepatol 2004; 2: pp. 905-911.
8. Park S.H., Lee S.S., Choi E.K., et. al.: Flat colorectal neoplasms: definition, importance, and visualization on CT colonography. AJR Am J Roentgenol 2007; 188: pp. 953-959.
9. Kim D.H., Pickhardt P.J., Taylor A.J., et. al.: CT colonography versus colonoscopy for the detection of advanced neoplasia. N Engl J Med 2007; 357: pp. 1403-1412.
10. Pickhardt P.J.: Screening CT colonography: how I do it. AJR Am J Roentgenol 2007; 189: pp. 290-298.
11. Pickhardt P.J., Nugent P.A., Choi J.R., et. al.: Flat colorectal lesions in asymptomatic adults: implications for screening with CT virtual colonoscopy. AJR Am J Roentgenol 2004; 183: pp. 1343-1347.
12. Rubesin S., Saul S., Laufer I., et. al.: Carpet lesions of the colon. Radiographics 1985; 5: pp. 537-552.
13. Tanaka S., Haruma K., Oka S., et. al.: Clinicopathologic features and endoscopic treatment of superficially spreading colorectal neoplasms larger than 20 mm. Gastrointest Endosc 2001; 54: pp. 62-66.
14. Pickhardt P.J., Lee A.D., McFarland E.G., et. al.: Linear polyp measurement at CT colonography: in vitro and in vivo comparison of two-dimensional and three-dimensional displays. Radiology 2005; 236: pp. 872-878.
15. Zalis M.E., Barish M.A., Choi J.R., et. al.: CT colonography reporting and data system: a consensus proposal. Radiology 2005; 236: pp. 3-9.
16. Pickhardt P.J., Choi J.R., Hwang I., et. al.: Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003; 349: pp. 2191-2200.
17. Muto T., Kamiya J., Sawada T., et. al.: Small flat adenoma of the large bowel with special reference to its clinicopathologic features. Dis Colon Rect 1985; 28: pp. 847-851.
18. Park S.H., Kim S.Y., Lee S.S., et. al.: Sensitivity of CT colonography for nonpolypoid colorectal lesions interpreted by human readers and with computer-aided detection. AJR Am J Roentgenol 2009; 193: pp. 70-78.
19. Dachman A.H., Zalis M.E.: Quality and consistency in CT colonography and research reporting. Radiology 2004; 230: pp. 319-323.
20. Soetikno R., Friedland S., Kaltenbach T., et. al.: Nonpolypoid (flat and depressed) colorectal neoplasms. Gastroenterology 2006; 130: pp. 566-576.
21. Fidler J., Johnson C.: Flat polyps of the colon: accuracy of detection by CT colonography and histologic significance. Abdom Imaging 2008; 34: pp. 157-171.
22. Karita M., Cantero D., Okita K.: Endoscopic diagnosis and resection treatment for flat adenoma with severe dysplasia. Am J Gastroenterol 1993; 88: pp. 1421-1423.
23. Kudo S.: Endoscopic mucosal resection of flat and depressed types of early colorectal-cancer. Endoscopy 1993; 25: pp. 455-461.
24. Watanabe T., Sawada T., Kubota Y., et. al.: Malignant potential in flat elevations. Dis Colon Rect 1993; 36: pp. 548-553.
25. Sakashita M., Aoyama N., Maekawa S., et. al.: Flat-elevated and depressed, subtypes of flat early colorectal cancers, should be distinguished by their pathological features. Int J Colorect Dis 2000; 15: pp. 275-281.
26. Suzuki N., Price A.B., Talbot I.C., et. al.: Flat colorectal neoplasms and the impact of the revised Vienna Classification on their reporting: a case-control study in UK and Japanese patients. Scand J Gastroenterol 2006; 41: pp. 812-819.
27. Rex D.K., Alikhan M., Cummings O., et. al.: Accuracy of pathologic interpretation of colorectal polyps by general pathologists in community practice. Gastrointest Endosc 1999; 50: pp. 468-474.
28. Costantini M., Sciallero S., Giannini A., et. al.: Interobserver agreement in the histologic diagnosis of colorectal polyps: the experience of the multicenter adenoma colorectal study (SMAC). J Clin Epidemiol 2003; 56: pp. 209-214.
29. Fidler J.L., Johnson C.D., MacCarty R.L., et. al.: Detection of flat lesions in the colon with CT colonography. Abdom Imaging 2002; 27: pp. 292-300.
30. Park S.H., Ha H.K., Kim A.Y., et. al.: Flat polyps of the colon: detection with 16-MDCT colonography—preliminary results. AJR Am J Roentgenol 2006; 186: pp. 1611-1617.
31. Park S.H., Ha H.K., Kim M.J., et. al.: False-negative results at multi-detector row CT colonography: multivariate analysis of causes for missed lesions. Radiology 2005; 235: pp. 495-502.
32. Taylor S.A., Iinuma G., Saito Y., et. al.: CT colonography: computer-aided detection of morphologically flat T1 colonic carcinoma. Eur Radiol 2008; 18: pp. 1666-1673.
33. Summers R.M., Liu J.M., Yao J.H., et. al.: Automated measurement of colorectal polyp height at CT colonography: hyperplastic polyps are flatter than adenomatous polyps. AJR Am J Roentgenol 2009; 193: pp. 1305-1310.
34. MacCarty R.L., Johnson C.D., Fletcher J.G., et. al.: Occult colorectal polyps on CT colonography: implications for surveillance. AJR Am J Roentgenol 2006; 186: pp. 1380-1383.
35. Pickhardt P.J., Choi J.R., Hwang I., et. al.: Nonadenomatous polyps at CT colonography: prevalence, size distribution, and detection rates. Radiology 2004; 232: pp. 784-790.
36. Baxter N.N., Goldwasser M.A., Paszat L.F., et. al.: Association of colonoscopy and death from colorectal cancer: a population-based, case-control study. Ann Intern Med 2008; 150: pp. 1-8.
37. Bressler B., Paszat L.F., Vinden C., et. al.: Colonoscopic miss rates for right-sided colon cancer: a population-based analysis. Gastroenterology 2004; 127: pp. 452-456.
38. Bond J.H.: Clinical relevance of the small colorectal polyp. Endoscopy 2001; 33: pp. 454-457.
39. Pickhardt P.J., Hassan C., Laghi A., et. al.: Cost-effectiveness of colorectal cancer screening with computed tomography colonography—the impact of not reporting diminutive lesions. Cancer 2007; 109: pp. 2213-2221.
40. Pickhardt P.J., Hassan C., Laghi A., et. al.: Small and diminutive polyps detected at screening CT colonography: a decision analysis for referral to colonoscopy. AJR Am J Roentgenol 2008; 190: pp. 136-144.
41. Pickhardt P.J., Nugent P.A., Mysliwiec P.A., et. al.: Location of adenomas missed by optical colonoscopy. Ann Intern Med 2004; 141: pp. 352-359.
42. Heresbach D., Barrioz T., Lapalus M.G., et. al.: Miss rate for colorectal neoplastic polyps: a prospective multicenter study of back-to-back video colonoscopies. Endoscopy 2008; 40: pp. 284-290.
43. Kanao H., Tanaka S., Oka S., et. al.: Narrow-band imaging magnification predicts the histology and invasion depth of colorectal tumors. Gastrointest Endosc 2009; 69: pp. 631-636.
44. Rastogi A., Pondugula K., Bansal A., et. al.: Recognition of surface mucosal and vascular patterns of colon polyps by using narrow-band imaging: interobserver and intraobserver agreement and prediction of polyp histology. Gastrointest Endosc 2009; 69: pp. 716-722.
45. Sikka S., Ringold D.A., Jonnalagadda S., et. al.: Comparison of white light and narrow band high definition images in predicting colon polyp histology, using standard colonoscopes without optical magnification. Endoscopy 2008; 40: pp. 818-822.
46. Kaltenbach T., Friedland S., Soetikno R.: A randomised tandem colonoscopy trial of narrow band imaging versus white light examination to compare neoplasia miss rates. Gut 2008; 57: pp. 1406-1412.
47. Adler A., Aschenbeck J., Yenerim T., et. al.: Narrow-band versus white-light high definition television endoscopic imaging for screening colonoscopy: a prospective randomized trial. Gastroenterology 2009; 136: pp. 410-416.
48. Stoffel E.M., Turgeon K., Stockwell D.H., et. al.: Chromoendoscopy detects more adenomas than colonoscopy using intensive inspection without dye spraying. Cancer Prevent Res 2008; 1: pp. 507-513.
49. Ratiu N., Gelbmann C., Rath H.C., et. al.: Chromoendoscopy with indigo carmine in flexible sigmoidoscopy screening: does it improve the detection of adenomas in the distal colon and rectum?. J Gastrointest Liver Dis 2007; 16: pp. 153-156.