
Rationale and Objectives
This study aimed to determine the utility of directed ultrasound and digital mammogram for evaluating focal breast pain in women with different mammographic breast densities.
Materials and Methods
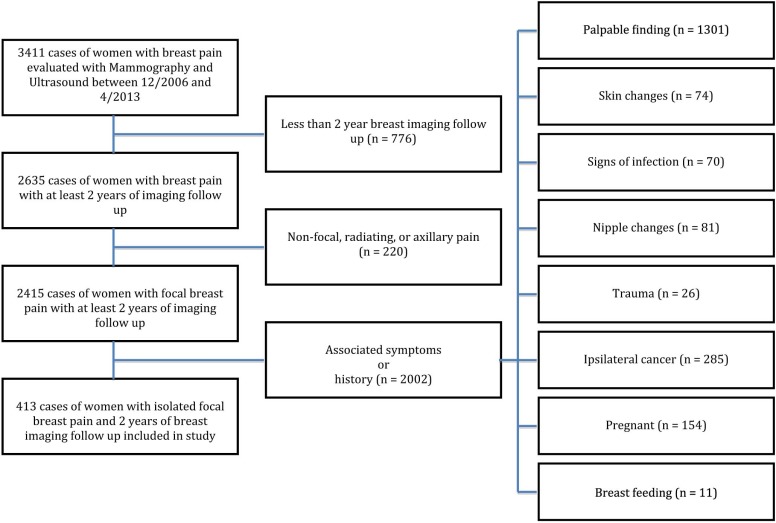
This institutional review board–approved and Health Insurance Portability and Accountability Act–compliant retrospective study included 413 cases of focal breast pain in 369 women (mean age 53 years). All cases were evaluated with both mammogram and ultrasound and had at least 2 years of imaging follow-up. Exclusion criteria were non-focal, axillary, or radiating pain; palpable or skin changes; pregnancy or lactation; and history of trauma or infection. Breast density, imaging findings, and biopsy results were recorded. Specificity, positive predictive values, and negative predictive values were calculated.
Results
Eighteen percent (76 of 413) of cases demonstrated an imaging correlate. Of these, 74% (56 of 76) occurred in dense breasts and 26% (20 of 76) in nondense breasts. Seventy percent (14 of 20) of lesions in nondense breasts were seen with mammography and ultrasound, whereas 30% (6 of 20) were detected only with ultrasound. Of lesions detected in dense breasts, 29% (16 of 56) were seen with mammography and ultrasound, whereas 71% (40 of 56) were detected only with ultrasound. Thirty-one percent (24 of 76) of cases were biopsied, 42% (10 of 24) of which were detected by ultrasound only. No cancer was detected in initial workup. At 2-year follow-up, three women, all with dense breasts, developed cancer in the same quadrant as the initial pain.
Conclusions
Directed ultrasound, when performed in conjunction with digital mammography for the evaluation of focal breast pain in women with nondense breasts, is of low utility and may contribute to unnecessary intervention as a result of incidental findings.
Introduction
Breast pain is one of the most common symptoms for which women seek medical care . Although up to 80% of women experience breast pain at some point in their lives, most commonly breast pain results from a benign etiology including idiopathic causes, simple cysts, trauma, infection, pregnancy, or lactation . In contrast, breast cancer is reported in up to 4% of women presenting with focal breast pain . Despite the uncommon association between breast cancer and focal breast pain, a diagnostic imaging workup can be requested . Current American College of Radiology Appropriateness Criteria guidelines rate the use of mammography and ultrasound for the evaluation of noncyclical, focal, unilateral, or bilateral breast pain in patients 30 years and older as “may be appropriate”; in women under 30, ultrasound is rated “may be appropriate” and mammography is rated “usually not appropriate” . Traditionally, both mammography and ultrasound are performed in women older than 30 years, who present with noncyclical, focal breast pain as imaging can often exclude a treatable benign cause of pain and/or provide reassurance .
However, current recommendations for imaging primary focal breast pain are controversial owing to the overall paucity of data limited by small sample sizes and short follow-up intervals . Furthermore, most studies include data obtained from film screen mammography, which has been replaced by digital mammography as the standard of care ( Table 1 ). One study to date has evaluated the utility of mammography over long follow-up intervals (average: 51 months), but this study included both screen film and digital mammograms . To our knowledge, there is no published work evaluating the utility of directed breast ultrasound in combination with digital mammography in a large study population over a long follow-up period. In addition, none of the previous work has assessed the utility of ultrasound in the setting of focal breast pain among women with different mammographic breast densities.
Table 1
Summary of Literature
Author Year Cohort Mean Duration of Follow-up No. of Cases with Benign Imaging Findings No. of Cases with Breast Cancer ( N ) (mo)N (%)N (%) Duijm et al. 1998 987 48 129(13) 4(0.4) Leddy et al. 2013 257 12 117(46) 3(1) Tumyan et al. 2005 86 26.5 82(95) \* 4(4.7) † Masroor et al. 2009 55(5 focal pain) 48 38(69) 0(0) Noroozian et al. 2015 617(304 focal pain) 51 63(10.2) 11(1.8) Leung et al. 2002 110 29 25(23) 0(0)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Patient Inclusion and Exclusion Criteria
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Technique
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Imaging
Get Radiology Tree app to read full this article<
Table 2
Imaging Findings in Women with Primary Focal Breast Pain
Modality Finding_N_ (%) Cases with imaging findings 76(100) Digital mammography 3(4) Calcifications 2(3) Asymmetry 1(1) Directed ultrasound 46(61) Cyst 32(42) Mass 8(11) Lymph node 3(4) Fibroadenoma 1(1) Fluid collection 1(1) Hypoechoic area 1(1) Digital mammography and directed ultrasound 27(36) Mass or asymmetry on digital mammogram found to be a cyst on directed ultrasound 14(18) Mass on digital mammogram found to be a milk duct on directed ultrasound 1(1) Postoperative change on digital mammography found to be a mass on directed ultrasound 1(1) Cyst 4(5) Mass 5(7) Silicone 2(3)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histology Results and Follow-up
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Description of Breast Cancer Detected on Follow-up
Age (y) 64 50 68 Duration of follow-up (mo) 12 50 32 Imaging indication Routine screening Routine screening Palpable abnormality Imaging finding Mammogram Cluster of pleomorphic calcifications with an associated irregular spiculated mass None 8 mm area of grouped punctate, round calcifications Ultrasound 1.5 cm × 1.5 cm × 1.2 cm mass with angular margins 1 cm × 0.8 cm × 1 cm irregular mass None Histology Invasive ductal carcinoma Invasive ductal carcinoma Ductal carcinoma in situ Nodal status None None None Stage 1 1 0 Grade 3 1 Nuclear grade 2
Get Radiology Tree app to read full this article<
Breast Density
Get Radiology Tree app to read full this article<
Table 4
Mammographic Breast Density
Mammographic Density Nondense Breast Dense Breast Total Cohort ( N ) 180 233 413 Cases with imaging findings, N (%) 20(26) 56(74) 76(100) Cases with findings only on ultrasound, N (%) 6(13) 40(87) 46(100) Cases with subsequent cancer development, N (%) 0(0) 3(100) 3(100)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Masroor I., Afzal S., Sakhawat S., et. al.: Negative predictive value of mammography and sonography in mastalgia with negative physical findings. J Pak Med Assoc 2009; 59: pp. 598-601.
2. Mansel R.: ABC of breast diseases: breast pain. BMJ 1994; 309: pp. 866-868.
3. Howard M., Battaglia T., Prout M., et. al.: The effect of imaging on the clinical management of breast pain. J Gen Intern Med 2012; 27: pp. 817-824.
4. Morrow M.: The evaluation of common breast problems. Am Fam Physician 2000; 61: pp. 2371-2378. 2385
5. Jokich P., Newell M.S., Bailey L., et. al.: ACR Appropriateness Criteria® breast pain. Available at: http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/BreastPain.pdf American College of Radiology; Accessed June 20, 2015
6. Barton M.: Breast symptoms among women enrolled in a health maintenance organization: frequency, evaluation, and outcome. Ann Intern Med 1999; 130: pp. 651.
7. Preece P.: Clinical syndromes of mastalgia. Lancet 1976; 308: pp. 670-673.
8. Srivastava A., Mansel R., Arvind N., et. al.: Evidence-based management of Mastalgia: a meta-analysis of randomised trials. Breast 2007; 16: pp. 503-512.
9. Harvey J.A., Mahoney M.C., Newell M.S., et. al.: ACR Appropriateness Criteria® palpable breast masses. Available at http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/PalpableBreastMasses.pdf American College of Radiology; Accessed June 20, 2015
10. Vaidyanathan L., Barnard K., Elnicki D.: Benign breast disease: when to treat, when to reassure, when to refer. Cleve Clin J Med 2002; 69: pp. 425-432.
11. Noroozian M., Stein L., Gaetke-Udager K., et. al.: Long-term clinical outcomes in women with breast pain in the absence of additional clinical findings: mammography remains indicated. Breast Cancer Res Treat 2015; 149: pp. 417-424.
12. Olcucuoglu E., Yilmaz G.: Mastodynia: is imaging necessary in young patients?. Turk J Surg 2013; pp. 17-19.
13. Tumyan L., Hoyt A., Bassett L.: Negative predictive value of sonography and mammography in patients with focal breast pain. Clin Imaging 2006; 30: pp. 147.
14. Leddy R., Irshad A., Zerwas E., et. al.: Role of breast ultrasound and mammography in evaluating patients presenting with focal breast pain in the absence of a palpable lump. Breast J 2013; 19: pp. 582-589.
15. Leung J., Kornguth P., Gotway M.: Utility of targeted sonography in the evaluation of focal breast pain. J Ultrasound Med 2002; 21: pp. 521-526.
16. Duijm L., Guit G., Hendriks J., et. al.: Value of breast imaging in women with painful breasts: observational follow up study. BMJ 1998; 317: pp. 1492-1495.
17. Millet A., Dirbas F.: Clinical management of breast pain: a review. Obstet Gynecol Surv 2002; 57: pp. 451-461.
18. Preece P., Mansel R., Hughes L.: Mastalgia: psychoneurosis or organic disease?. BMJ 1978; 1: pp. 29-30.
19. Pisano E., Hendrick R., Yaffe M., et. al.: Diagnostic accuracy of digital versus film mammography: exploratory analysis of selected population subgroups in DMIST 1. Radiology 2008; 246: pp. 376-383.
20. American College of Radiology : Breast imaging reporting and data system (BI-RADS).4th ed.2003.American College of RadiologyReston, VA