
Rationale and Objectives
Fluid-attenuated inversion recovery (FLAIR) imaging can detect elevated protein levels in fluid that may be difficult or impossible to detect with T1- or T2-weighted imaging. The purpose of this study is to evaluate the frequency and asses the diagnostic utility of abnormal FLAIR signal in various types of inner ear and internal auditory canal (IAC) pathology.
Materials and Methods
A retrospective review of medical records and magnetic resonance images from 187 consecutive patients who underwent imaging of the temporal bones for possible inner ear or IAC pathology over a 1-year period were reviewed for abnormal increased FLAIR signal, increased intrinsic T1 signal, abnormal enhancement after gadolinium administration, and the presence of a mass lesion within the cerebellopontine angle, IAC, or inner ear. Reviewers were blinded to clinical diagnosis.
Results
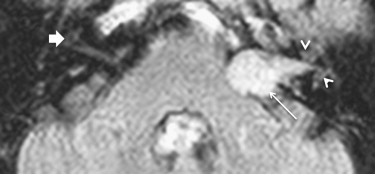
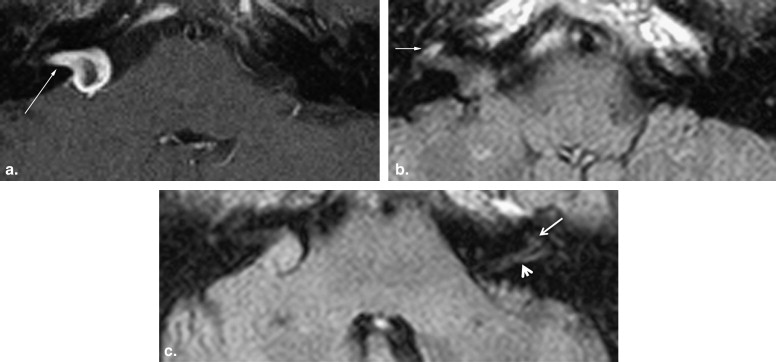
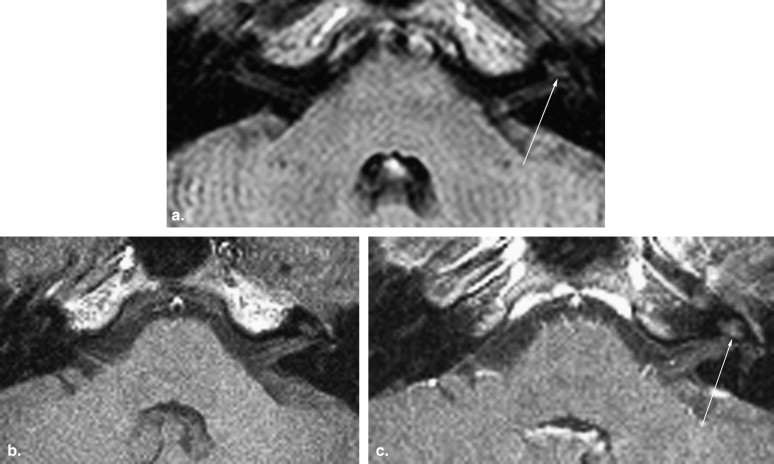
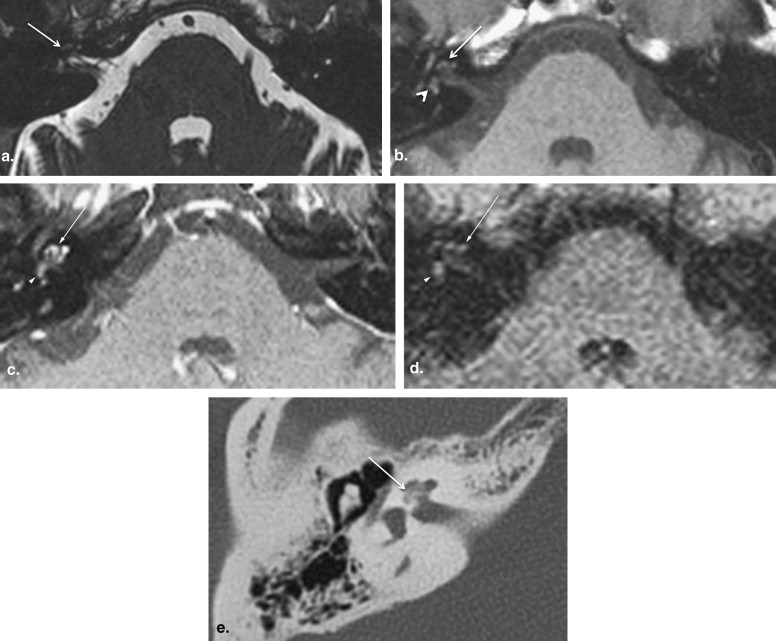
Twenty-five of 32 (78%) patients with schwannomas restricted to the IAC and cerebellopontine angle demonstrated associated increased FLAIR signal within the ipsilateral inner ear structures. The sensitivity, specificity, positive predictive value, and negative predictive value of inner ear FLAIR hyperintensity for a schwannoma were 80%, 95%, 78%, and 95%, respectively. Inner ear FLAIR hyperintensity was also seen in cases of intracochlear hemorrhage, labyrinthitis, and labyrinthitis ossificans, but these conditions did not occur with sufficient frequency in our study population to determine statistical significance.
Conclusion
Identification of inner ear FLAIR hyperintensity can alert the radiologist to scrutinize pre- and post-gadolinium T1-weighted images and T2-weighted images for subtle IAC and inner ear abnormalities. Although enhancement after the administration of gadolinium contrast media is the gold standard for detection of schwannoma, inner ear FLAIR hyperintensity may be a helpful diagnostic adjunct for vestibular schwannoma. This may be particularly helpful when gadolinium was not administered and the T2-weighted images are equivocal, especially when dedicated thin-section imaging of the IACs and temporal bones was not performed.
The fluid-attenuated inversion recovery (FLAIR) pulse sequence nulls signal from cerebrospinal fluid and produces T2-weighted images. It has been shown to detect elevated protein levels, hemorrhage, and other cerebrospinal fluid abnormalities that are difficult or impossible to detect with standard T1- or T2-weighted imaging . Although inner ear FLAIR signal abnormality has been described in a number of conditions including schwannomas, labyrinthitis, and in cases of deafness from mumps (paramyxovirus) infection, the frequency of this finding and its potential utility as a secondary marker for various types of internal auditory canal (IAC) or inner ear pathology has not been fully described . In our study, we evaluated the frequency of IAC and inner ear FLAIR hyperintensity in various types of IAC and inner ear pathology by studying a series of consecutive patients who underwent dedicated magnetic resonance imaging (MRI) of the temporal bone for a variety of clinical indications.
Materials and methods
The study was conducted as a retrospective review of medical records and MRI studies. The reviewers were blinded to the clinical history and diagnosis.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Clinical Diagnoses and Inner Ear FLAIR Hyperintensity
Clinical Diagnosis for Cause of Symptoms that Prompted Magnetic Resonance Imaging Examination Number of Patients Number of Patients with Inner Ear Fluid-attenuated Inversion Recovery Hyperintensity Vestibular schwannoma 35 28 Endolymphatic hydrops 9 0 Benign paroxysmal positional vertigo 5 0 Noise-induced hearing loss 5 0 Migraine-associated vertigo 4 0 Presbycusis 4 0 Otitis media/eustachian tube dysfunction 3 0 Labyrinthitis 3 1 Barotrauma 2 0 Remote trauma 2 0 Vancomycin vestibulopathy 1 0 Presumed cochlear hemorrhage 1 1 Labyrinthitis ossificans 1 1 Petrous apex granuloma 1 0 Orthostatic hypotension 1 0 Vascular compression 1 0 Meningioma 1 0 Hyperacusis/stapedius reflex 1 0 Attic cholesteatoma 1 0 Bell’s palsy 1 0 Rubella-related hearing loss 1 0 High-riding jugular bulb 1 0 Otosclerosis 1 0 Inflammatory paranasal sinus disease 1 0 Postsurgical changes of transmastoid surgery 1 1 Multiple sclerosis and/or sarcoidosis 1 0 Migraines and benign paroxysmal positional vertigo 1 0 Endolymphatic hydrops and benign paroxysmal positional vertigo 1 0 No final clinical diagnosis in medical record to explain patient’s symptoms 97 3 Total 187 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Inner Ear FLAIR Hyperintensity and Presence or Absence of Schwannoma
Schwannoma No Schwannoma Inner ear FLAIR hyperintensity 28 8 No inner ear FLAIR hyperintensity 7 144
FLAIR, fluid-attenuated inversion recovery.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Otake H., Sugiura M., Naganawa S., et. al.: 3D-FLAIR magnetic resonance imaging in the evaluation of mumps deafness. Int J Pediatr Otorhinolaryngol 2006; 70: pp. 2115-2117.
2. Bhadelia R.A., Tedesco K.L., Hwang S., et. al.: Increased cochlear fluid-attenuated inversion recovery signal in patients with vestibular schwannoma. AJNR Am J Neuroradiol 2008; 29: pp. 720-723.
3. Sugiura M., Naganawa S., Teranishi M., et. al.: Three-dimensional fluid-attenuated inversion recovery magnetic resonance imaging findings in patients with sudden sensorineural hearing loss. Laryngoscope 2006; 116: pp. 1451-1454.
4. Allen R.W., Harnsberger H.R., Shelton C., et. al.: Low-cost high-resolution fast spin-echo MR of acoustic schwannoma: an alternative to enhanced conventional spin-echo MR?. AJNR Am J Neuroradiol 1996; 17: pp. 1205-1210.
5. Harnsberger H.R., Shelton C.: Mass screening for retrocochlear disorders. AJNR Am J Neuroradiol 2002; 23: pp. 897-898.
6. Asaoka K., Barrs D.M., Sampson J.H., et. al.: Intracanalicular meningioma mimicking vestibular schwannoma. AJNR Am J Neuroradiol 2002; 23: pp. 1493-1496.
7. Melhem E.R., Jara H., Eustace S.: Fluid-attenuated inversion recovery MR imaging: identification of protein concentration threshold for CSF hyperintensity. AJR Am J Roentgenol 1997; 169: pp. 859-862.
8. O’Connor A.F., France M.W., Morrison A.W.: Perilymph total protein levels associated with cerebellopontine angle lesions. Am J Otol 1981; 2: pp. 193-195.
9. Fukui M.B., Weissman J.L., Curtin H.D., et. al.: T2-weighted MR characteristics of internal auditory canal masses. AJNR Am J Neuroradiol 1996; 17: pp. 1211-1218.
10. Jackler R.K.: Cost-effective screening for acoustic neuroma with unenhanced MR: a clinician’s perspective. AJNR Am J Neuroradiol 1996; 17: pp. 1226-1228.
11. Hegarty J.L., Patel S., Fischbein N., et. al.: The value of enhanced magnetic resonance imaging in the evaluation of endocochlear disease. Laryngoscope 2002; 112: pp. 8-17.
12. Jagannathan J., Butman J.A., Lonser R.R., et. al.: Endolymphatic sac tumor demonstrated by intralabyrinthine hemorrhage. Case report. J Neurosurg 2007; 107: pp. 421-425.
13. Weissman J.L., Hisch B.E., Fukui M.B., et. al.: The evolving MR appearance of structures in the internal auditory canal after removal of an acoustic neuroma. AJNR Am J Neuroradiol 1997; 18: pp. 313-323.
14. Palacios E., Valvassori G.: Hemorrhagic labyrinthitis. Ear Nose Throat J 2000; 79: pp. 80.
15. Brodie H.A., Thompson T.C., Vassilian L., et. al.: Induction of labyrinthitis ossificans after pneumococcal meningitis: an animal model. Otolaryngol Head Neck Surg 1998; 118: pp. 15-21.