
Rationale and Objectives
To compare prospectively 64-detector-row computed tomographic colonography (CTC) after a full-laxative tagging-based preparation (full preparation) with a minimum-laxative tagging-based preparation (minimum preparation) with respect to diagnostic performance in the detection of polyps, tagging quality, and patient acceptance.
Materials and Methods
Consecutive 101 patients at high risk for developing colorectal cancer were alternately assigned to either a full preparation group (n = 51) or a minimum preparation group (n = 50) for fecal-tagging CTC. The full preparation consisted of administration of 2-L polyethylene glycol solution with 20 mL of sodium diatrizoate for fecal tagging. The minimum preparation consisted of ingestion of a total of 45 mL of sodium diatrizoate during the 3 days before and 10 mL of sodium picosulfate solution the night before CT. Colonoscopy was used as the reference standard. We assessed the accuracy of polyp detection and the tagging quality for each preparation. All patients were given questionnaires related to their acceptance.
Results
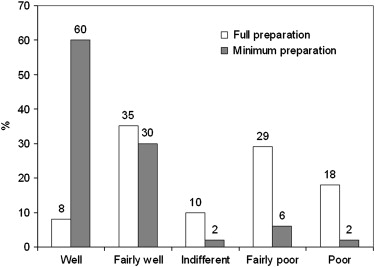
Per-patient sensitivity, specificity, and positive and negative predictive values for polyps ≥ 6 mm were as follows: full preparation group, 97%, 92%, 88%, and 98%, respectively; minimum preparation group, 88%, 68%, 56%, and 92%, respectively. Average visual subjective tagging scores for the full and minimum preparation groups were 94.6% and 76.1%, respectively ( P < .0001). Minimum preparation was better tolerated than full preparation.
Conclusion
Although full-laxative and minimum-laxative fecal-tagging CTC yielded an equally high sensitivity in the detection of polyps ≥ 6 mm, the full-laxative fecal-tagging CTC yielded a better specificity than did the minimum-laxative fecal-tagging CTC. Thus, it is desirable to offer patients an option of either full-laxative fecal-tagging CTC for highest diagnostic accuracy and ability to perform a same-day therapeutic colonoscopy without additional bowel preparation, or minimum-laxative fecal-tagging CTC for those unwilling to undergo full preparation but willing to accept moderate decrease in specificity.
Currently, two types of bowel preparation with fecal tagging are used for computed tomographic colonography (CTC) . The first type is designed to reduce the cleansing procedure as much as possible with fecal tagging for improving patient compliance and acceptance of the preparation . The second type is a conventional, full-laxative preparation with fecal tagging for achieving the cleanest possible colon to yield the best results for polyp detection regardless of patients’ diet or bowel habits . Although clinical trials have been conducted with each bowel preparation regimen, a single trial comparing these two bowel preparation regimens with fecal tagging on a consecutive cohort of patients has not been reported.
Our purpose in this study was prospectively to compare conventional full-laxative with minimum-laxative fecal-tagging CTC in terms of diagnostic performance in the detection of polyps, tagging quality, and patient acceptance in a consecutive patient cohort using 64-detector-row CT scanning.
Materials and methods
Patients and Study Design
Get Radiology Tree app to read full this article<
Bowel Preparation for CTC
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics
Characteristics Full Preparation (n = 51) Minimum Preparation (n = 50)P Value Mean age, years ± SD 54.8 ± 15.1 55.4 ± 12.8 0.90 Gender, W/M 16/35 24/26 0.13 Clinical indication to be eligible for examination of total colon (%) 0.44 Hematochezia 19 (37%) 14 (28%) Fecal occult blood 32 (63%) 36 (72%)
Data are numbers of patients, unless otherwise indicated.
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Colonography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Colonoscopy
Get Radiology Tree app to read full this article<
Reference Standard
Get Radiology Tree app to read full this article<
Patient Questionnaire
Get Radiology Tree app to read full this article<
Table 2
Questionnaire Pertaining to Patient Tolerance and Preference
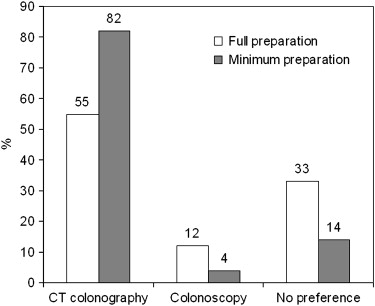
(For full-laxative tagging-based preparation group) How did you tolerate the full-laxative tagging-based preparation before CT colonography and optical colonoscopy? 1; Well, 2; Fairly well, 3; Indifferent, 4; Fairly poor, 5; Poor (For minimum-laxative tagging-based preparation group) How did you tolerate the minimum-laxative tagging-based preparation before CT colonography? 1; Well, 2; Fairly well, 3; Indifferent, 4; Fairly poor, 5; Poor How did you find the minimum-laxative tagging-based preparation before CT colonography compared with the PEG-based standard pre-colonoscopy preparation? 1; Much better, 2; Better, 3; No difference, 4; Worse, 5; Much worse (For both groups) Since you had both CT colonography and colonoscopy: which examination would you repeat in the future? 1; CT colonography, 2; Colonoscopy, 3; No preference
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Colonoscopic and Histopathologic Findings
Get Radiology Tree app to read full this article<
Table 3
Size and Histopathology Distribution of Polyps by Bowel Preparation Type
Full Preparation Minimum Preparation Number of all polyps 78 34 Number of polyps ≥ 6 mm 32 23 Size (mean ± SD) 8.30 ± 13.6 mm 10.8 ± 12.4 mm Size (distribution) <6 mm 46 (59%) 11 (32%) 6–9 mm 17 (22%) 14 (41%) ≥10 mm 15 (19%) 9 (27%) Histopathology of polyps ≥ 6 mm (distribution) Hyperplastic lesion 4 (13%) 5 (22%) Adenoma 21 (66%) 14 (61%) Cancer 7 (22%) 4 (17%)
Data are polyp numbers, unless otherwise indicated.
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group; SD, standard deviation.
Get Radiology Tree app to read full this article<
Tagging Quality
Get Radiology Tree app to read full this article<
Diagnostic Performance in the Detection of Polyps on CTC
Get Radiology Tree app to read full this article<
Table 4
Per-Patient Diagnostic Performance in the Detection of Polyps ≥ 6 mm
Sensitivity Specificity PPV NPV Overall 93% (98–77) 80% (88–67) 71% (82–54) 95% (99–85) Full preparation 97% (100–74) 92% (98–75) 88% (97–64) 98% (100–83) Minimum preparation 88% (98–62) 68% (83–50) 56% (76–35) 92% (99–74)P value 0.11 0.0005 0.0008 0.11
Data are averages of the performance of the two readers. Numbers in parentheses are 95% confidence intervals.
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group; PPV, positive predictive value; NPV, negative predictive value.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Per-Polyp Diagnostic Performance in the Detection of Polyps ≥ 6 mm
TP FN FP Sensitivity_P_ Value PPV_P_ Value Overall 6–9 mm 25.5 5.5 17 82 (93–63)% 60 (74–43)% ≥10 mm 24 0 3 100 (100–88)% 89 (98–71)% 6–9 mm .49 .013 Full preparation 14.5 2.5 5 85 (96–57)% 74 (91–49)% Minimum preparation 11 3 12 79 (95–49)% 48 (67–29)% ≥10 mm 1.0 .0037 Full preparation 15 0 0 100 (100–82)% 100 (100–82)% Minimum preparation 9 0 3 100 (100–72)% 75 (95–43)% ≥6 mm .37 .0002 Full preparation 29.5 2.5 5 92 (98–75)% 86 (95–69)% Minimum preparation 20 3 15 87 (97–66)% 57 (74–41)%
Data are averages of the numbers of lesions resulting from the two readers, unless otherwise indicated. Numbers in parentheses are 95% confidence intervals.
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group; TP, true-positive; FN, false-negative; FP, false-positive; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 6
Causes for False-Positive Findings in Per-Polyp Diagnostic Performance
Total Number Partially Tagged Stool Untagged Stool Fold Thickening Full preparation Reader 1 6 1 0 5 Reader 2 4 0 0 4 Minimum preparation Reader 1 17 7 4 6 Reader 2 13 7 2 4
Data are numbers of false-positive findings.
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group.
Table 7
Causes for False-Negative Findings in Per-Polyp Diagnostic Performance
Total Number Perceptual Error Submerged Polyp in Inhomogeneously Tagged Stool No clear Cause ∗ Full preparation Reader 1 2 2 0 0 Reader 2 3 3 0 0 Minimum preparation Reader 1 2 0 1 1 Reader 2 4 2 1 1
Data are numbers of false-negative findings.
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group.
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 8
Agreement between Readers Regarding the Identification of Patients with Colorectal Polyps (Per-Patient for Polyps ≥ 6 mm) and the Presence or Absence of Individual Colorectal Polyps (Per-Polyp ≥ 6 mm)
Per-Patient Per-Polyp Overall 0.90 (0.072) 0.55 (0.075) Full preparation 0.93 (0.12) 0.43 (0.11) Minimum preparation 0.88 (0.094) 0.57 (0.10)
Data are κ coefficients (± standard error). Agreement is considered fair to good if κ values are 0.4–0.75 and excellent if greater than 0.75 . A κ value of zero indicates absence of agreement; negative κ values indicate disagreement .
Full preparation, full-laxative tagging-based preparation group; minimum preparation, minimum-laxative tagging-based preparation group.
Get Radiology Tree app to read full this article<
Patient Tolerance and Preference
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Pickhardt P.J.: CT colonography without catharsis: the ultimate study or useful additional option?. Gastroenterology 2005; 128: pp. 521-522.
2. Nagata K., Näppi J., Cai W., et. al.: Minimum-invasive early diagnosis of colorectal cancer with CT colonography: techniques and clinical value. Expert Opin Med Diagn 2008; 2: pp. 1233-1246.
3. Bielen D., Thomeer M., Vanbeckevoort D., et. al.: Dry preparation for virtual CT colonography with fecal tagging using water-soluble contrast medium: initial results. Eur Radiol 2003; 13: pp. 453-458.
4. Lefere P., Gryspeerdt S., Baekelandt M., et. al.: Laxative-free CT colonography. AJR Am J Roentgenol 2004; 183: pp. 945-948.
5. Iannaccone R., Laghi A., Catalano C., et. al.: Computed tomographic colonography without cathartic preparation for the detection of colorectal polyps. Gastroenterology 2004; 127: pp. 1300-1311.
6. Johnson K.T., Carston M.J., Wentz R.J., et. al.: Development of a cathartic-free colorectal cancer screening test using virtual colonoscopy: a feasibility study. AJR Am J Roentgenol 2007; 188: pp. W29-W36.
7. Zalis M.E., Perumpillichira J.J., Magee C., et. al.: Tagging-based, electronically cleansed CT colonography: evaluation of patient comfort and image readability. Radiology 2006; 239: pp. 149-159.
8. Pickhardt P.J., Choi J.R., Hwang I., et. al.: Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003; 349: pp. 2191-2200.
9. Kim D.H., Pickhardt P.J., Hinshaw J.L., et. al.: Prospective blinded trial comparing 45-mL and 90-mL doses of oral sodium phosphate for bowel preparation before computed tomographic colonography. J Comput Assist Tomogr 2007; 31: pp. 53-58.
10. Nagata K., Endo S., Ichikawa T., et. al.: Polyethylene glycol solution (PEG) plus contrast medium vs PEG alone preparation for CT colonography and conventional colonoscopy in preoperative colorectal cancer staging. Int J Colorectal Dis 2007; 22: pp. 69-76.
11. Sugiyama A., Ohashi Y., Gomi A., et. al.: Colorectal screening with single scan CT colonography in children. Pediatr Surg Int 2007; 23: pp. 987-990.
12. Morrin M.M., Farrell R.J., Keogan M.T., et. al.: CT colonography: colonic distention improved by dual positioning but not intravenous glucagon. Eur Radiol 2002; 12: pp. 525-530.
13. Bruzzi J.F., Moss A.C., Brennan D.D., et. al.: Efficacy of IV Buscopan as a muscle relaxant in CT colonography. Eur Radiol 2003; 13: pp. 2264-2270.
14. Pickhardt P.J.: Screening CT colonography: how I do it. AJR Am J Roentgenol 2007; 189: pp. 290-298.
15. Jeong J.Y., Kim M.J., Kim S.S.: Manual and automated polyp measurement comparison of CT colonography with optical colonoscopy. Acad Radiol 2008; 15: pp. 231-239.
16. Lefere P.A., Gryspeerdt S.S., Dewyspelaere J., et. al.: Dietary fecal tagging as a cleansing method before CT colonography: initial results polyp detection and patient acceptance. Radiology 2002; 224: pp. 393-403.
17. Callstrom M.R., Johnson C.D., Fletcher J.G., et. al.: CT colonography without cathartic preparation: feasibility study. Radiology 2001; 219: pp. 693-698.
18. Snedecor G.W., Cochran W.G.: Statistical methods.8th ed.1989.Iowa State University PressAmes, IA
19. Fleiss J.L.: The measurement of inter-rater agreement.statistical methods for rates and proportions.1981.John WileyNew York, NY:pp. 212-236.
20. Johnson C.D., Chen M.H., Toledano A.Y., et. al.: Accuracy of CT colonography for detection of large adenomas and cancers. N Engl J Med 2008; 359: pp. 1207-1217.
21. Jensch S., de Vries A.H., Pot D., et. al.: Image quality and patient acceptance of four regimens with different amounts of mild laxatives for CT colonography. AJR Am J Roentgenol 2008; 191: pp. 158-167.
22. Jensch S., de Vries A.H., Peringa J., et. al.: CT colonography with limited bowel preparation: performance characteristics in an increased-risk population. Radiology 2008; 247: pp. 122-132.
23. Choi H.K., Chu K.W., Law W.L.: Therapeutic value of gastrografin in adhesive small bowel obstruction after unsuccessful conservative treatment: a prospective randomized trial. Ann Surg 2002; 236: pp. 1-6.
24. Kealey S.M., Dodd J.D., MacEneaney P.M., et. al.: Minimal preparation computed tomography instead of barium enema/colonoscopy for suspected colon cancer in frail elderly patients: an outcome analysis study. Clin Radiol 2004; 59: pp. 44-52.
25. Taylor S.A., Slater A., Burling D.N., et. al.: CT colonography: optimization, diagnostic performance and patient acceptability of reduced-laxative regimens using barium-based fecal tagging. Eur Radiol 2008; 18: pp. 32-42.
26. Miller S.H.: Anaphylactoid reaction after oral administration of diatrizoate meglumine and diatrizoate sodium solution. AJR Am J Roentgenol 1997; 168: pp. 959-961.
27. Seymour C.W., Pryor J.P., Gupta R., et. al.: Anaphylactoid reaction to oral contrast for computed tomography. J Trauma 2004; 57: pp. 1105-1107.
28. Kojima M., Wakai K., Tokudome S., et. al.: Bowel movement frequency and risk of colorectal cancer in a large cohort study of Japanese men and women. Br J Cancer 2004; 90: pp. 1397-1401.
29. Adibi P., Behzad E., Pirzadeh S., et. al.: Bowel habit reference values and abnormalities in young Iranian healthy adults. Dig Dis Sci 2007; 52: pp. 1810-1813.
30. Zutshi M., Hull T.L., Bast J., et. al.: Female bowel function: the real story. Dis Colon Rectum 2007; 50: pp. 351-358.
31. Ristvedt S.L., McFarland E.G., Weinstock L.B., et. al.: Patient preferences for CT colonography, conventional colonoscopy, and bowel preparation. Am J Gastroenterol 2003; 98: pp. 578-585.
32. Kim S.H., Choi B.I., Han J.K., et. al.: CT colonography in a Korean population with a high residue diet: comparison between wet and dry preparations. Clin Radiol 2006; 61: pp. 483-494.
33. Davis G.R., Santa Ana C.A., Morawski S.G., et. al.: Inhibition of water and electrolyte absorption by polyethylene glycol (PEG). Gastroenterology 1980; 79: pp. 35-39.
34. Poon C.M., Lee D.W., Mak S.K., et. al.: Two liters of polyethylene glycol-electrolyte lavage solution versus sodium phosphate as bowel cleansing regimen for colonoscopy: a prospective randomized controlled trial. Endoscopy 2002; 34: pp. 560-563.
35. Ell C., Fischbach W., Keller R., et. al.: A randomized, blinded, prospective trial to compare the safety and efficacy of three bowel-cleansing solutions for colonoscopy (HSG-01 ∗ ). Endoscopy 2003; 35: pp. 300-304.
36. Mathus-Vliegen E.M., Kemble U.M.: A prospective randomized blinded comparison of sodium phosphate and polyethylene glycol-electrolyte solution for safe bowel cleansing. Aliment Pharmacol Ther 2006; 23: pp. 543-552.
37. Näppi J., Okamura A., Frimmel H., et. al.: Region-based supine-prone correspondence for the reduction of false-positive CAD polyp candidates in CT colonography. Acad Radiol 2005; 12: pp. 695-707.
38. Nappi J., Yoshida H.: Fully automated three-dimensional detection of polyps in fecal-tagging CT colonography. Acad Radiol 2007; 14: pp. 287-300.
39. Zalis M.E., Barish M.A., Choi J.R., et. al.: CT colonography reporting and data system: a consensus proposal. Radiology 2005; 236: pp. 3-9.
40. Pickhardt P.J., Hassan C., Laghi A., et. al.: Cost-effectiveness of colorectal cancer screening with computed tomography colonography: the impact of not reporting diminutive lesions. Cancer 2007; 109: pp. 2213-2221.
41. Kim D.H., Pickhardt P.J., Taylor A.J., et. al.: CT colonography versus colonoscopy for the detection of advanced neoplasia. N Engl J Med 2007; 357: pp. 1403-1412.