
Rationale and Objectives
Several minimally invasive thermal techniques have been developed for the treatment of benign thyroid nodules. A new technique for this indication is high-intensity focused ultrasound (HIFU). The aim of this study was to assess effectiveness in varying preablative nodule volumes and whether outcome patterns that were reported during studies with other thermal ablative procedures for thyroid nodule ablation would also apply to HIFU.
Materials and Methods
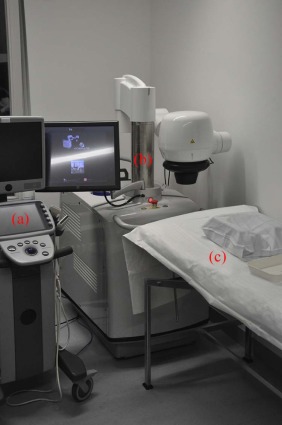
Over the last 2 years, 19 nodules in 15 patients (12 women) whose average age was 58.7 years (36–80) were treated with HIFU in an ambulatory setting. Patients with more than one nodule were treated in multiple sessions on the same day. The mean nodule volume was 2.56 mL (range 0.13–7.67 mL). The therapeutic ultrasound probe (Echopulse THC900888-H) used in this series functions with a frequency of 3 MHz, reaching temperatures of approximately 80°C–90°C and delivering an energy ranging from 87.6 to 320.3 J per sonication. To assess the effectiveness of thermal ablation, nodular volume was measured at baseline and at 3-month follow-up. The end point of the study was the volume reduction assessment after 3 months’ follow-up. Therapeutic success was defined as volume reduction of more than 50% compared to baseline. This study was retrospectively analyzed using the Wilcoxon signed rank test and Kendall tau.
Results
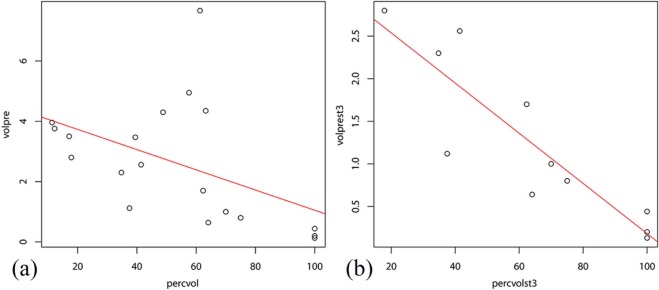
The median percentage volume reduction of all 19 nodules after 3 months was 58%. An inverse correlation between preablative nodular volume and percentage volume shrinking was found (tau = −0.46, P < .05). Therapeutic success was achieved in 10 out of 19 patients (53%).
Conclusions
HIFU of benign thyroid nodules can be carried out as an alternative therapy for nodules ≤3 mL if patients are refusing surgery or radioiodine therapy.
Introduction
Despite its small size, the thyroid gland receives great medical attention. To our current knowledge, variability multitude of pathologies are present in the gland itself, that is, thyroid cancer, hormone balance complaints, Graves disease, Hashimoto disease, nodular goiter, iodine deficiency goiter, and thyroid nodules. The last mentioned are divided into benign, malignant, hypofunctional, and hyperfunctional nodules and can be diagnosed quite precisely with modern equipment . Benign thyroid nodules are showing a wide prevalence, and the standard therapy options for collateral symptoms are surgery—most frequently hemithyroidectomy and thyroidectomy—or radioiodine therapy . Both therapies have their advantages but hold several drawbacks. The most common are life-lasting hypothyreosis, infections, and other iatrogenic injuries for surgical intervention and hypothyreosis, infections, and endocrinopathy for radioiodine therapy . In addition, radioiodine therapy is in principle available only for treating hyperfunctional nodules, whereas surgical intervention is often recommended for hypofunctional nodules or cysts even though modern diagnostic methods are able to exclude malignancy and, therefore, suggesting less harmful therapy for symptomatic nodules . Considering all these facts, research investigated alternatives that do not share these disadvantages, and several minimally invasive techniques were developed for treating benign thyroid nodules. New promising alternatives are ethanol sclerotherapy , radiofrequency ablation , microwave ablation , laser ablation , and high-intensity focused ultrasound (HIFU) . Most of these therapy options were assessed intensively over the past years, leading to significant results, which converted them in routine clinical practice . However, HIFU, which is the least invasive and at the same time the most precise technique, still needs more detailed data concerning the treatment of the thyroid gland . Our workgroup assessed several ablative techniques including HIFU . To add complementary data related to this new technique, our research was focused on investigating characteristics regarding effectiveness that occurred in other minimally invasive techniques , and determine factors that allow a precise prognosis of therapy success. As nodule volume is the crucial assessment parameter of both treatment success and patient comfort, the main criterion of judgment was volume evaluation. The author especially aimed to search if a negative correlation between preablative nodule volume and percentage of volume reduction could be established and to determine a threshold volume value that implies a limitation related to a single HIFU session.
Materials and Methods
Study Design
This is a retrospective analysis of data generated in a single-arm, open-label, baseline-controlled study. The study complied with institutional review board, ethics committees, informed consent regulations, International Committee on Harmonization Good Clinical Practice Guidelines, the Declaration of Helsinki, and local regulations. The treatment protocol detailed by Korkusuz et al. was used in this study .
Patients
Get Radiology Tree app to read full this article<
Treatment Procedure and Equipment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Baseline Assessment and End Points
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
Efficacy and Therapeutic Success
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Declarations
Ethics Approval and Consent to Participate
Get Radiology Tree app to read full this article<
Availability of Data and Material
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Giovanella L., Suriano S., Maffioli M., et. al.: (99m)Tc-sestamibi scanning in thyroid nodules with nondiagnostic cytology. Head Neck 2010; 32: pp. 607-611.
2. Reiners C., Schumm-Draeger P.M., Geling M., et. al.: Schilddrüsenultraschallscreening (Initiative Papillon). Internist 2003; 44: pp. 412-419.
3. Schicha H., Hellmich M., Lehrmacher W., et. al.: Should all patients with thyroid nodules ≥ 1 cm undergo fine-needle aspiration biopsy?. Nuklearmedizin 2009; 48: pp. 79-83.
4. Schmid K.W., Sheu S.-Y., Görges R., et. al.: Tumoren der Schilddrüse. Pathologe 2003; 24: pp. 357-372.
5. Völzke H., Lüdemann J., Robinsn D.M., et. al.: The prevalence of undiagnosed thyroid disorders in a previously iodine-deficient area. Thyroid 2003; 13: pp. 803-810.
6. Happel C., Truong P.N., Bockisch B., et. al.: Colour-coded duplex-sonography versus scintigraphy. Can scintigraphy be replaced by sonography for diagnosis of functional thyroid autonomy?. Nuklearmedizin 2013; 52: pp. 157-203.
7. Korkusuz H., Happel C., Heck K., et. al.: Percutaneous thermal microwave ablation of thyroid nodules. Nuklearmedizin 2014; 53: pp. 123-130.
8. Jeong W.K., Baek J.H., Rhim H., et. al.: Radiofrequency ablation of benign thyroid nodules: safety and imaging follow-up in 236 patients. Eur Radiol 2008; 18: pp. 1244-1250.
9. Na D.G., Lee J.H., Jung S.L., et. al.: Korean Society of Thyroid Radiology (KSThR); Korean Society of Radiology. Radiofrequency ablation of benign thyroid nodules and recurrent thyroid cancers: consensus statement and recommendations. Korean J Radiol 2012; 13: pp. 117-125.
10. Dietlein M., Dressler J., Grünwald F., et. al.: Leitlinie zur Radioiodtherapie (RIT) bei benignen Schilddrüsenerkrankungen (Version 4). Nuklearmedizin 2007; 46: pp. 220-223.
11. Lin C.M., Doyle P., Tsan Y.T., et. al.: 131 I treatment for thyroid cancer and risk of developing primary hyperparathyroidism: a cohort study. Eur J Nucl Med Mol Imaging 2014; 41: pp. 253-259.
12. Christou N., Mathonnet M.: Complications after total thyroidectomy. J Visc Surg 2013; 150: pp. 249-256.
13. Martino E., Murtas M.L., Loviselli A., et. al.: Percutaneous intranodular ethanol injection for treatment of autonomously functioning thyroid nodules. Surgery 1992; 112: pp. 1161-1165.
14. Korkusuz H., Happel C., Grünwald F.: Ultrasound guided percutaneous microwave ablation of hypofunctional thyroid nodules: evaluation by scintigraphic 99mTc-MIBI imaging. Nuklearmedizin 2013; 52: pp. 205-257.
15. Yue W., Wang S., Wang B., et. al.: Ultrasound guided percutaneous microwave ablation of benign thyroid nodules: safety and imaging follow-up in 222 patients. Eur J Radiol 2013; 82: pp. e11-e16.
16. Pacella C.M., Mauri G., Achille G., et. al.: Outcomes and risk factors for complications of laser ablation for thyroid nodules: a multicenter study on 1531 patients. J Clin Endocrinol Metab 2015; 100: pp. 3903-3910.
17. Mauri G., Cova L., Monaco C.G., et. al.: Benign thyroid nodules treatment using percutaneous laser ablation (PLA) and radiofrequency ablation (RFA). Int J Hyperthermia 2016; 15: pp. 1-5.
18. Mainini A.P., Monaco C., Pescatori L.C., et. al.: Image-guided thermal ablation of benign thyroid nodules. J Ultrasound 2016; 20: pp. 11-22.
19. Mauri G., Sconfienza L.M.: Percutaneous ablation holds the potential to substitute for surgery as first choice treatment for symptomatic benign thyroid nodules. Int J Hyperthermia 2016; 22: pp. 1-2.
20. Pacella C.M., Mauri G., Cesareo R., et. al.: A comparison of laser with radiofrequency ablation for the treatment of benign thyroid nodules: a propensity score matching analysis. Int J Hyperthermia 2017; 12: pp. 1-9.
21. Korkusuz H., Fehre N., Sennert M., et. al.: Early assessment of high-intensity focused ultrasound treatment of benign thyroid nodules by scintigraphic means. J Ther Ultrasound 2014; 2: pp. 18.
22. Korkusuz H., Sennert M., Fehre N., et. al.: Local thyroid tissue ablation by high-intensity focused ultrasound: effects on thyroid function and first human feasibility study with hot and cold thyroid nodules. Int J Hyperthermia 2014; 30: pp. 480-485.
23. Korkusuz H., Fehre N., Sennert M., et. al.: Volume reduction of benign thyroid nodules 3 months after a single treatment with high-intensity focused ultrasound (HIFU). J Ther Ultrasound 2015; 3: pp. 4.
24. Korkusuz H., Sennert M., Fehre N., et. al.: Localized thyroid tissue ablation by high intensity focused ultrasound: volume reduction, effects on thyroid function and immune response. Rofo 2015; 187: pp. 1011-1015.
25. Esnault O., Rouxel A., Le Nestour E., et. al.: Minimally invasive ablation of a toxic thyroid nodule by high-intensity focused ultrasound. AJNR Am J Neuroradiol 2010; 31: pp. 1967-1968.
26. Esnault O., Franc B., Ménégaux F., et. al.: High-intensity focused ultrasound ablation of thyroid nodules: first human feasibility study. Thyroid 2011; 21: pp. 965-973.
27. Kovatcheva R.D., Vlahov J.D., Stoinov J.I., et. al.: Benign solid thyroid nodules: US-guided high-intensity focused ultrasound ablation-initial clinical outcomes. Radiology 2015; 276: pp. 597-605.
28. Korkusuz H., Happel C., Koch D.A., et. al.: Combination of ultrasound-guided percutaneous microwave ablation and radioiodine therapy in benign thyroid disease: A 3-month follow-up study. Rofo 2016; 188: pp. 60-68.
29. Heck K., Happel C., Grünwald F., et. al.: Percutaneous microwave ablation of thyroid nodules: effects on thyroid function and antibodies. Int J Hyperthermia 2015; 31: pp. 560-567.
30. Happel C., Korkusuz H., Koch D.A., et. al.: Combination of ultrasound guided percutaneous microwave ablation and radioiodine therapy in benign thyroid diseases. A suitable method to reduce the 131I activity and hospitalization time?. Nuklearmedizin 2015; 54: pp. 118-124.
31. Korkusuz H., Nimsdorf F., Happel C., et. al.: Percutaneous microwave ablation of benign thyroid nodules. Functional imaging in comparison to nodular volume reduction at a 3-month follow-up. Nuklearmedizin 2015; 54: pp. 13-19.
32. Korkusuz H., Happel C., Heck K., et. al.: Percutaneous thermal microwave ablation of thyroid nodules. Preparation, feasibility, efficiency. Nuklearmedizin 2014; 53: pp. 123-130.
33. R Core Team : R: A language and environment for statistical computing.2013.R Foundation for Statistical ComputingVienna, Austria ISBN 3-900051-07 http://www.R-project.org/
34. Bhuyan B.K.: Kinetics of cell kill by hyperthermia. Cancer Res 1979; 39: pp. 2277-2284.
35. Pérez-López F.R., Ornat L., Ceausu I., et. al.: EMAS position statement: management of uterine fibroids. Maturitas 2014; 79: pp. 106-116. pii: S0378-5122(14)00198-4
36. Rewcastle J.C.: High intensity focused ultrasound for prostate cancer: a review of the scientific foundation, technology and clinical outcomes. Technol Cancer Res Treat 2006; 5: pp. 619-625.
37. Illing R.O., Kennedy J.E., Wu F., et. al.: The safety and feasibility of extracorporeal high-intensity focused ultrasound (HIFU) for the treatment of liver and kidney tumors in a Western population. Br J Cancer 2005; 93: pp. 890-895.
38. Kovatcheva R., Guglielmina J.N., Abehsera M., et. al.: Ultrasound-guided high-intensity focused ultrasound treatment of breast fibroadenoma—a multicenter experience. J Ther Ultrasound 2015; 3: pp. 1.
39. Lang B.H., Woo Y.C., Chiu K.W.: Single-session high-intensity focused ultrasound treatment in large-sized benign thyroid nodules. Thyroid 2017; 27: pp. 714-721. Epub 2017 Mar 22
40. Lang B.H., Woo Y.C., Wong C.K.H.: High-intensity focused ultrasound for treatment of symptomatic benign thyroid nodules: a prospective study. Radiology 2017; 18: pp. 161640.
41. Lang B.H.H., Wong C.K.H., Ma E.P.M.: Single-session high intensity focussed ablation (HIFU) versus open cervical hemithyroidectomy for benign thyroid nodule: analysis on early efficacy, safety and voice quality. Int J Hyperthermia 2017; 24: pp. 1-7.
42. Lang B.H.H., Woo Y.C., Chiu K.W.: High-intensity focused ablation (HIFU) of single benign thyroid nodule rarely alters underlying thyroid function. Int J Hyperthermia 2017; 24: pp. 1-7.
43. Mauri G., Cova L., Ierace T., et. al.: Treatment of metastatic lymph nodes in the neck from papillary thyroid carcinoma with percutaneous laser ablation. Cardiovasc Intervent Radiol 2016; 39: pp. 1023-1030.
44. Durante C., Costante G., Lucisano G., et. al.: The natural history of benign thyroid nodules. JAMA 2015; 313: pp. 926-935.