
Rationale and Objectives
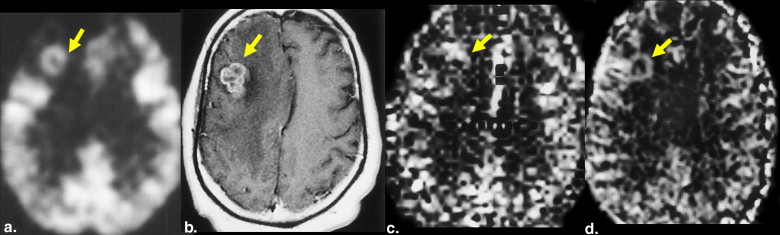
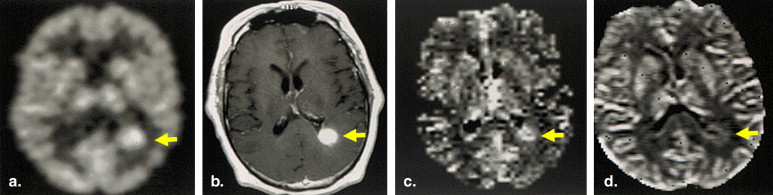
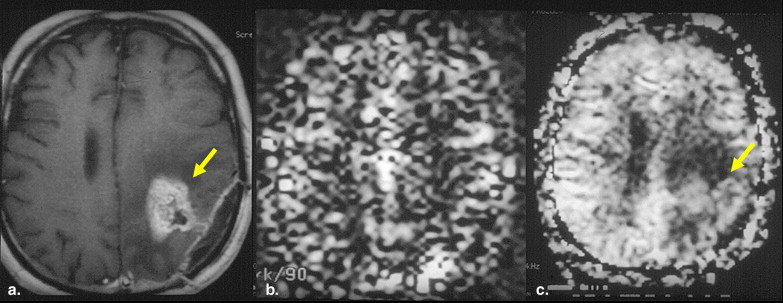
Distinguishing recurrent glial tumor from radiation necrosis can be challenging. The purpose of this pilot study was to preliminarily compare unenhanced arterial spin-labeled (ASL) imaging, dynamic susceptibility contrast-enhanced cerebral blood volume (DSCE-CBV) magnetic resonance imaging, and positron emission tomographic (PET) imaging in distinguishing predominant glioma recurrence or progression from predominant radiation necrosis in postoperative patients treated with proton-beam therapy.
Methods
Patients with grade II to IV glioma previously treated with surgery and proton-beam therapy were enrolled on the basis of new enhancing nodules or masses with primary differential diagnoses of predominant tumor recurrence or progression versus radiation necrosis. ASL, DSCE-CBV, and PET examinations were assessed by visual qualitative and quantitative analysis for the detection of predominant tumor recurrence. Imaging results were correlated with a clinical-pathologic reference standard.
Results
Thirty patients were studied, resulting in 33 ASL, 32 DSCE-CBV, and 26 PET examinations. On the basis of visual inspection, the sensitivities of PET, ASL, and DSCE-CBV examinations for detecting high-grade tumor foci were 81%, 88%, and 86%, respectively. The highest sensitivity values for quantitative ASL imaging were obtained using a normalized cutoff ratio of 1.3, resulting in sensitivity of 94% for ASL imaging and 71% for DSCE-CBV imaging. When predominant high-grade tumors with superimposed regions of predominant mixed radiation necrosis were excluded, DSCE-CBV sensitivity improved to 90%, but ASL sensitivity remained unchanged.
Conclusions
Compared with DSCE-CBV imaging, ASL imaging may more accurately distinguish predominant recurrent high-grade glioma from radiation necrosis, especially in regions with mixed radiation necrosis, for which DSCE-CBV imaging may underestimate true blood volume because of leakage artifacts.
Primary central nervous system neoplasia is one of the most frequent causes of death between 15 and 35 years of age . Gliomas constitute >90% of primary brain tumors diagnosed after the second decade of life . Despite treatment with chemotherapy and radiation, including proton-beam therapy (PBT) and other radiosurgery, the majority of these tumors progress and/or recur. Moreover, treatment with radiation remains associated with tissue necrosis that may also lead to clinical deterioration . When a magnetic resonance imaging (MRI) scan of the brain shows a new enhancing lesion after a patient has undergone surgery and radiation for high-grade glioma, the differentiation of predominant recurrent tumor (or progression of tumor) from predominant radiation necrosis is often crucial, because the two entities have different treatment approaches and prognoses .
Computed tomographic and conventional MRI findings are relatively nonspecific, although some findings on MRI, especially when presenting in combination, may favor a given diagnosis . Positron emission tomographic (PET) and single photon-emission computed tomographic imaging provide additional information regarding tumor metabolism . Although early results with fluorodeoxyglucose (FDG) PET imaging were encouraging, some studies have reported specificities as low as 18%, high cost, and limited availability . Glioma recurrence or progression and radiation necrosis may be frequently mixed (in terms of pathology), and residual microscopic tumor foci are often present, even in so-called pure necrosis cases, further complicating the situation .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Enrollment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Brain Tumors
Get Radiology Tree app to read full this article<
Clinical Follow-Up
Get Radiology Tree app to read full this article<
PET Examinations
Get Radiology Tree app to read full this article<
MRI Examinations
Get Radiology Tree app to read full this article<
ASL Imaging
Get Radiology Tree app to read full this article<
DSCE-CBV Imaging
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Distribution of Sensitivity and Specificity Values of Predominantly Recurrent or Progressive Versus Nonrecurrent High-grade Tumor
Modality Total Nonrecurrence Recurrence Sensitivity Specificity ASL imaging 33 12 (36%) 21 (64%) 88% 89% DSCE-CBV imaging 32 10 (33%) 22 (67%) 86% 70% PET imaging 26 12 (46%) 14 (54%) 81% 90% Histopathology 35 12 (34%) 23 (66%)
ASL, arterial spin-labeled; DSCE-CBV, dynamic susceptibility contrast-enhanced cerebral blood volume; PET, positron emission tomographic.
The findings are based on grading scores on three-point scale for ASL, DSCE-CBV, and PET imaging in patients treated with proton-beam therapy (Friedman’s test, P < .01 for all three comparisons). Consensus rating scores of 0 and 1 indicated nonrecurrence, whereas a score of 2 indicated high-grade recurrence.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
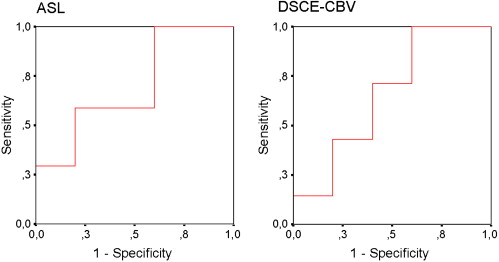
Table 2
Test Characteristics for the Detection of Predominant Recurrent or Progressive High-Grade Glioma in PBT-treated Patients, Based on Quantitative ROI Analyses, Applying a Cutoff Ratio of 1.3
ASL Imaging DSCE-CBV Imaging With Mixed Histology Without Mixed Histology With Mixed Histology Without Mixed Histology Variable ( n = 23) ( n = 18) ( n = 19) ( n = 15) Sensitivity 94% 92% 71% 90% Specificity 50% 50% 40% 40% PPV 88% 85% 77% 75% NPV 12% 15% 15% 16%
ASL, arterial spin-labeled; DSCE-CBV, dynamic susceptibility contrast-enhanced cerebral blood volume, NPV, negative predictive value; PBT, proton-beam therapy; PPV, positive predictive value; ROI, region of interest.
The second and fourth columns represent patients excluding mixed high-grade tumor and radiation necrosis.
Table 3
Mean Normalized ROI Values Based on Quantitative ROI Analyses of the Perfusion Map Values, Stratified According to Clinical-pathologic Diagnoses
Normalized ROI ASL Imaging DSCE-CBV Imaging Histopathology ( n = 23) ( n = 19) Predominant radiation necrosis/low-grade tumor 2.0 ± 1.4 ( n = 5) 2 ± 1.5 ( n = 5) Predominant high-grade tumor recurrence 3.9 ± 5 ( n = 13) 2.6 ± 1.8 ( n = 10) Radiation necrosis with mixed high-grade tumor 4.3 ± 1.6 ( n = 5) 1.2 ± 0.3 ( n = 4)
The differences between the nonrecurrence and predominantly high-grade recurrence for histopathologic subgroups were not statistically significant (Student’s t test).
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Langleben D.D., Segall G.M.: PET in differentiation of recurrent brain tumor from radiation injury. J Nucl Med 2000; 41: pp. 1861-1867.
2. Kleihues P., Soylemezoglu F., Schauble B., et. al.: Histopathology, classification, and grading of gliomas. Glia 1995; 15: pp. 211-221.
3. Bénard F., Romsa J., Hustinx R.: Imaging gliomas with positron emission tomography and single-photon emission computed tomography. Semin Nucl Med 2003; 33: pp. 148-162.
4. Loeffler J.S., Alexander E., Hochberg F.H., et. al.: Clinical patterns of failure following stereotactic interstitial irradiation for malignant gliomas. Int J Radiat Oncol Biol Phys 1990; 19: pp. 1455-1462.
5. Mullins M.E., Barest G.D., Schaefer P.W., et. al.: Radiation necrosis versus glioma recurrence: conventional MR imaging clues to diagnosis. AJNR Am J Neuroradiol 2005; 26: pp. 1967-1972.
6. Valk P.E., Dillon W.P.: Radiation injury of the brain. AJNR Am J Neuroradiol 1991; 12: pp. 45-62.
7. Ricci P.E., Karis J.P., Heiserman J.E., et. al.: Differentiating recurrent tumor from radiation necrosis: time for re-evaluation of positron emission tomography?. AJNR Am J Neuroradiol 1998; 19: pp. 407-413.
8. Kahn D., Follett K.A., Bushnell D.L., et. al.: Diagnosis of recurrent brain tumor: value of 201Tl SPECT vs 18F-fluorodeoxyglucose PET. AJR Am J Roentgenol 1994; 163: pp. 1459-1465.
9. Kumar A.J., Leeds N.E., Fuller G.N., et. al.: Malignant gliomas: MR imaging spectrum of radiation therapy- and chemotherapy-induced necrosis of the brain after treatment. Radiology 2000; 217: pp. 377-384.
10. Roberts H.C., Roberts T.P., Brasch R.C., et. al.: Quantitative measurement of microvascular permeability in human brain tumors achieved using dynamic contrast-enhanced MR imaging: correlation with histologic grade. AJNR Am J Neuroradiol 2000; 21: pp. 891-899.
11. Roberts H.C., Roberts T.P., Bollen A.W., et. al.: Correlation of microvascular permeability derived from dynamic contrast-enhanced MR imaging with histologic grade and tumor labeling index: a study in human brain tumors. Acad Radiol 2001; 8: pp. 384-391.
12. Lemort M., Canizares-Perez A.C., Van der Stappen A., Kampouridis S.: Progress in magnetic resonance imaging of brain tumours. Curr Opin Oncol 2007; 19: pp. 616-622.
13. Nelson S.J., Cha S.: Imaging glioblastoma multiforme. Cancer J 2003; 9: pp. 134-145.
14. Puduvalli V.K., Sawaya R.: Antiangiogenesis—therapeutic strategies and clinical implications for brain tumors. J Neurooncol 2000; 50: pp. 189-200.
15. Folkman J.: The role of angiogenesis in tumor growth. Semin Cancer Biol 1992; 3: pp. 65-71.
16. Okunieff P., Dols S., Lee J., et. al.: Angiogenesis determines blood flow, metabolism, growth rate, and ATPase kinetics of tumors growing in an irradiated bed: 31P and 2H nuclear magnetic resonance studies. Cancer Res 1991; 51: pp. 3289-3295.
17. Estrada G., González-Maya L., Celis-López M.A., et. al.: Diagnostic approach in suspected recurrent primary brain tumors using (18)FDG-PET/MRI, perfusion MRI, visual and quantitative analysis, and three dimensional stereotactic surface projections. First experience in Mexico. Rev Esp Med Nucl 2008; 27: pp. 329-339.
18. Sugahara T., Korogi Y., Tomiguchi S., et. al.: Posttherapeutic intraaxial brain tumor: the value of perfusion-sensitive contrast-enhanced MR imaging for differentiating tumor recurrence from nonneoplastic contrast-enhancing tissue. AJNR Am J Neuroradiol 2000; 21: pp. 901-909.
19. Fuss M., Wenz F., Scholdei R., et. al.: Radiation-induced regional cerebral blood volume (rCBV) changes in normal brain and low-grade astrocytomas: quantification and time and dose-dependent occurrence. Int J Radiat Oncol Biol Phys 2000; 48: pp. 53-58.
20. Lev M.H., Ozsunar Y., Henson J.W., et. al.: Glial tumor grading and outcome prediction using dynamic spin-echo MR susceptibility mapping compared with conventional contrast-enhanced MR: confounding effect of elevated rCBV of oligodendroglimoas. AJNR Am J Neuroradiol 2004; 25: pp. 214-221.
21. Fitzek M.M., Thornton A.F., Rabinov J.D., et. al.: Accelerated fractionated proton/photon irradiation to 90 cobalt gray equivalent for glioblastoma multiforme: results of a phase II prospective trial. J Neurosurg 1999; 91: pp. 251-260.
22. Fitzek M.M., Thornton A.F., Harsh G.T., et. al.: Dose-escalation with proton/photon irradiation for Daumas-Duport lower-grade glioma: results of an institutional phase I/II trial. Int J Radiat Oncol Biol Phys 2001; 51: pp. 131-137.
23. Pardo F.S., Aronen H.J., Fitzek M., et. al.: Correlation of FDG-PET interpretation with survival in a cohort of glioma patients. Anticancer Res 2004; 24: pp. 2359-2365.
24. Aronen H.J., Pardo F.S., Kennedy D.N., et. al.: High microvascular blood volume is associated with high glucose uptake and tumor angiogenesis in human gliomas. Clin Cancer Res 2000; 6: pp. 2189-2200.
25. Kwong K.K., Chesler D.A., Weisskoff R.M., et. al.: MR perfusion studies with T1-weighted echo planar imaging. Magn Reson Med 1995; 34: pp. 878-887.
26. Petersen E.T., Zimine I., Ho Y.C., Golay X.: Non-invasive measurement of perfusion: a critical review of arterial spin labelling techniques. Br J Radiol 2006; 79: pp. 688-701.
27. Aronen H.J., Gazit I.E., Louis D.N., et. al.: Cerebral blood volume maps of gliomas: comparison with tumor grade and histologic findings. Radiology 1994; 191: pp. 41-51.
28. Weisskoff R., Rosen B.R.: Functional magnetic resonance imaging. Acad Radiol 1995; pp. 133-135.
29. Lev M.H., Rosen B.R.: Clinical applications of intracranial perfusion MR imaging. Neuroimaging Clin North Am 1999; 9: pp. 309-331.
30. Provenzale J.M., Wang G.R., Brenner T., Petrella J.R., Sorensen A.G.: Comparison of permeability in high-grade and low-grade brain tumors using dynamic susceptibility contrast MR imaging. AJR Am J Roentgenol 2002; 178: pp. 711-716.
31. Covarrubias D.J., Rosen B.R., Lev M.H.: Dynamic magnetic resonance perfusion imaging of brain tumors. Oncologist 2004; 9: pp. 528-537.
32. Song C.W., Lokshina A., Rhee J.G.: Implication of blood flow in hyperthermic treatment of tumors. IEEE Trans Biomed Eng 1984; 31: pp. 9-16.
33. Sadeghi N., Salmon I., Tang B.N., et. al.: Correlation between dynamic susceptibility contrast perfusion MRI and methionine metabolism in brain gliomas: preliminary results. J Magn Reson Imagin 2006; 24: pp. 989-994.
34. Spampinato M.V., Smith J.K., Kwock L., et. al.: Cerebral blood volume measurements and proton MR spectroscopy in grading of oligodendroglial tumors. AJR Am J Roentgenol 2007; 188: pp. 204-212.
35. Knopp E.A., Cha S., Johnson G., et. al.: Glial neoplasms: dynamic contrast-enhanced T2∗-weighted MR imaging. Radiology 1999; 211: pp. 791-798.
36. Uematsu H., Maeda M., Sadato N., et. al.: Blood volume of gliomas determined by double-echo dynamic perfusion-weighted MR imaging: a preliminary study. AJNR Am J Neuroradiol 2001; 22: pp. 1915-1919.
37. Aronen H.J., Perkio J.: Dynamic susceptibility contrast MRI of gliomas. Neuroimaging Clin North Am 2002; 12: pp. 501-523.
38. Warmuth C., Gunther M., Zimmer C.: Quantification of blood flow in brain tumors: comparison of arterial spin labeling and dynamic susceptibility-weighted contrast-enhanced MR imaging. Radiology 2003; 228: pp. 523-532.
39. Dean B.L., Drayer B.P., Bird C.R., et. al.: Gliomas: classification with MR imaging. Radiology 1990; 174: pp. 411-415.
40. Bagley L.J., Grossman R.I., Judy K.D., et. al.: Gliomas: correlation of magnetic susceptibility artifact with histologic grade. Radiology 1997; 202: pp. 511-516.
41. Miralbell R., Lomax A., Russo M.: Potential role of proton therapy in the treatment of pediatric medulloblastoma/primitive neuro-ectodermal tumors: spinal theca irradiation. Int J Radiat Oncol Biol Phys 1997; 38: pp. 805-811.
42. Forsyth P.A., Kelly P.J., Cascino T.L., et. al.: Radiation necrosis or glioma recurrence: is computer-assisted stereotactic biopsy useful?. J Neurosurg 1995; 82: pp. 436-444.
43. Pauliah M., Saxena V., Haris M., Husain N., Rathore R.K., Gupta R.K.: Improved T(1)-weighted dynamic contrast-enhanced MRI to probe microvascularity and heterogeneity of human glioma. Magn Reson Imaging 2007; 25: pp. 1292-1299.
44. Sugahara T., Korogi Y., Kochi M., et. al.: Correlation of MR imaging-determined cerebral blood volume maps with histologic and angiographic determination of vascularity of gliomas. AJR Am J Roentgenol 1998; 171: pp. 1479-1486.
45. Aronen H.J., Glass J., Pardo F.S., et. al.: Echo-planar MR cerebral blood volume mapping of gliomas. Clinical utility. Acta Radiol 1995; 36: pp. 520-528.
46. Wolf R.L., Wang J., Wang S., et. al.: Grading of CNS neoplasms using continuous arterial spin labeled perfusion MR imaging at 3 Tesla. J Magn Reson Imaging 2005; 22: pp. 475-482.
47. Gasparetto E.L., Pawlak M.A., Patel S.H., et. al.: Posttreatment recurrence of malignant brain neoplasm: accuracy of relative cerebral blood volume fraction in discriminating low from high malignant histologic volume fraction. Radiology 2009; 250: pp. 887-896.
48. Calamante F., Thomas D.L., Pell G.S., et. al.: Measuring cerebral blood flow using magnetic resonance imaging techniques. J Cereb Blood Flow Metab 1999; 19: pp. 701-735.
49. Cavuşoğlu M., Pfeuffer J., Uğurbil K., Uludağ K.: Comparison of pulsed arterial spin labeling encoding schemes and absolute perfusion quantification. Magn Reson Imaging 2009; 27: pp. 1039-1045.
50. Gevers S., Majoie C.B., van den Tweel X.W., Lavini C., Nederveen A.J.: Acquisition time and reproducibility of continuous arterial spin-labeling perfusion imaging at 3 T. AJNR Am J Neuroradiol 2009; 30: pp. 968-971.