
Rationale and Objectives
To measure perceptions of radiology residents regarding the imaging needs of the developing world and the potential role of an organized global health imaging curriculum during residency training.
Materials and Methods
An electronic survey was created and then distributed to residents in accredited US radiology residency.
Results
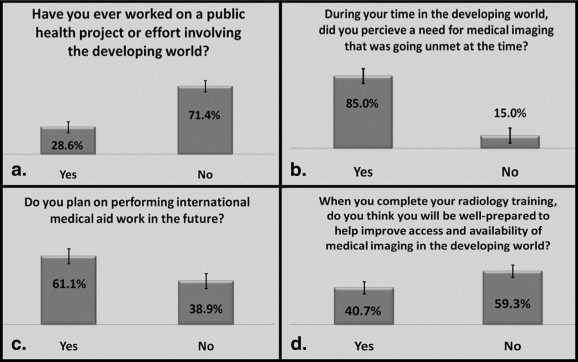
Two hundred ninety-four residents responded to the survey. A majority (61%) planned to pursue future international medical aid work, even though a similar proportion (59%) believed that they would be ill-prepared with their current training to pursue this career goal. The vast majority (91%) of respondents stated that their residency program offers no opportunities to participate in global health imaging experiences. Most surveyed residents felt that an organized global health imaging curriculum would improve understanding of basic disease processes (87%) and cost-conscious care (82%), prepare residents for lifelong involvement in global health (80%), and increase interpretative skills in basic radiology modalities (73%). If such a curriculum were available, most (62%) of surveyed residents stated that they would be likely or very likely to participate. Many (58%) believed the availability of such a program would have influenced their choice of residency program; a similar proportion of residents (75%) believed that the availability of a global health imaging curriculum would increase recruitment to the field of radiology.
Conclusion
Many radiology residents are motivated to acquire global health imaging experience, with most survey respondents planning to participate in global health initiatives. These data demonstrate an imbalance between the level of resident interest and the availability of global health imaging opportunities, and support the need for discussion on how to implement global health imaging training within radiology residency programs.
As globalization progresses, there is increasing agreement among medical educators that global health should be a standard component of general medical education in the United States . There is also a growing need for medical specialists in global health efforts, particularly as an increasing number of academic, government, and nongovernment organizations expand delivery of health care to developing nations in efforts to address the marked inequities in disease burden relative to health care expenditure ( Fig 1 ). Radiology is an important component of global public health programs, including those that address tuberculosis, AIDS-related diseases, trauma, breast cancer screening, and maternal-infant health care. Yet, the World Health Organization reports that approximately two thirds of the world’s population lacks adequate access to medical imaging; the scarcity of imaging services in developing regions contributes to a widening disparity of health care and limits the role of radiology in global public health programs that require imaging . Efforts to redress this lack of access to imaging services in the developing world have encountered significant challenges, including limited access to equipment, poor sustainability, shortages of trained personnel, inadequate infrastructure, and lack of interest .
 Open full size image
Open full size image
Figure 1
Graphical representation of health care inequities in the developing world.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Participants
Get Radiology Tree app to read full this article<
Instrument
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis
Get Radiology Tree app to read full this article<
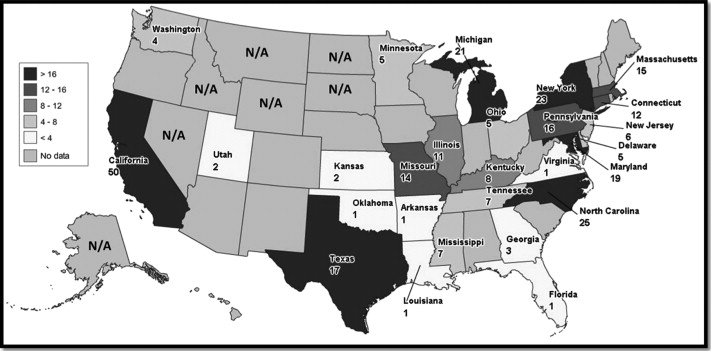
Table 1
Geographic Distribution of Radiology Resident Sample Population Relative to Actual Radiology Resident Population (ie, Does the Geographic Distribution of Surveyed Residents Mirror the Real Geographic Distribution of Radiology Residents?)
Subregion Region West (%) Midwest (%) South (%) Northeast (%) Pacific (CA, WA, OR, AK, HI) 7.1 Mountain (WY, ID, MT, NV, UT, CO, AZ, NM) −2.3 West North Central (ND, SD, NE, KS, MO, IA, MN) −1.8 East North Central (WI, MI, IL, IN, OH) −2.0 West South Central (TX, OK, AR, LA) −2.5 East South Central (MS, AL, KY, TN) 2.5 South Atlantic (FL, GA, SC, NC, VA, DC, MD, WV, DE) 5.9 Middle Atlantic (PA, NY, NJ) −6.5 New England (ME, VT, NH, CT, MA, RI) −0.4 Totals 4.8 −3.8 5.8 −6.9
Based on this analysis, we oversampled the West and South and undersampled the Midwest and Northeast; however, there was no significant association between region and the survey responses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Prior Experience
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Perceptions on Radiology’s Role in Global Health
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Participation in Global Health and Training Opportunities
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Global Health Imaging Curriculum and Clinical Rotation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 5, Survey responses regarding (a) likelihood of participation in international imaging during residency, respondents with prior experience more likely to have higher median score, confidence intervals based on sample size of 188 (responded to question), resident population of 4669 (from American College of Radiology [ACR]), and confidence level of 95%. (b) Possible effects of an international curriculum on resident recruitment to radiology, respondents with prior experience more likely to have higher median score, confidence intervals based on sample size of 190 (responded to question), resident population of 4669 (from ACR), and confidence level of 95%. (c) Effect of an international radiology curriculum on residency choice, respondents with prior experience more likely to have higher median score; confidence intervals based on sample size of 191 (responded to question), resident population of 4669 (from ACR), and confidence level of 95%. (d) The importance of an international elective rotation as a part of an international radiology curriculum, respondents with prior experience more likely to have higher median score, confidence intervals based on sample size of 189 (responded to question), resident population of 4669 (from ACR), and confidence level of 95%.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/GlobalHealthTraininginRadiologyResidencyPrograms/3_1s20S1076633211000894.jpg)
Table 2
Application of ACGME Core Competencies in a Global Health Imaging Elective Clinical Rotation
ACGME Competency Global Health Imaging Medical Knowledge Exposure to new clinical diseases in multiple modalities Patient Care Improving patient care through imaging consultation, screening, and direct imaging intervention Professionalism Adapting to providing care in low-resource health care systems to underserved populations Interpersonal and Communication Skills Cultural competency, communication, and clinical applications in a new cultural context;learning from and educating new clinical colleagues Practice-based Learning and Improvement Application of clinical skills to a new environment and disease processes, learning new imaging applications in developing world clinical settings Systems-based Practice Exposure to developing world practice environment and understanding low-resource cost-conscious care
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Challenges
Get Radiology Tree app to read full this article<
Table 3
Respondent Awareness Regarding Funding for an International Elective Rotation
Regarding an international radiology elective rotation, are you aware of possible funding sources? Answer Options Response (%) Response Count 95% CI No 88.5 201 ±4% Yes, through my training program 2.2 5 ±1.9% Yes, through my affiliated university graduated medical 3.1 7 ±2.2% Yes, through various radiological societies (eg, American College of Radiology, Radiological Society of North America) 5.7 13 ±2.9% Yes, through multiple sources 2.2 5 ±2.2%
Confidence intervals are as follows based on sample size (227), resident population of 4669 (from American College of Radiology), and confidence level of 95%.
Table 4
Potential Goals for Radiology Rotation
Which goals (if any) listed below do you believe that an international radiology curriculum during residency would achiever? (check all that apply) Answer Options Response (%) Response Count 95% CI Increased interpretive skill in basic radiology 72.5 161 ±5.7% Increased understanding of cost-conscious care 82.0 182 ±4.9% Increased understanding of diverse disease 87.8 195 ±4.2% Preparing residents for lifelong international radiology 80.6 179 ±5.1% Others (please specify) 1.8 4 ±1.7%
Confidence intervals are as follows based on sample size (222), resident population of 4669 (from American College of Radiology), and confidence level of 95%. “Other” category text responses included: Exposure to disease processes less commonly seen in the United States, perspective and professional fulfillment, my program sees almost no tuberculosis or HIV patients, I’m struggling to find opportunities for charity within the field of radiology, improved understanding of cultural restraints on imaging.
Get Radiology Tree app to read full this article<
Subgroup Analyses for Residents with Differences in Prior International Experience
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ayieko P., Akumu A.O., Griffiths U.K., et. al.: The economic burden of inpatient paediatric care in Kenya: household and provider costs for treatment of pneumonia, malaria and meningitis. Cost Eff Resour Alloc 2009; 7: pp. 3.
2. Ayieko P., English M.: Case management of childhood pneumonia in developing countries. Pediatr Infect Dis J 2007; 26: pp. 432-440.
3. World Health Organization. Diagnostic Imaging. World Health Organization Department of Essential Health Technologies, 2010. Available at: http://www.who.int/diagnostic_imaging/en . Accessed November 4, 2010.
4. Patel A., Mamtani M., Hibberd P.L., et. al.: Value of chest radiography in predicting treatment response in children aged 3–59 months with severe pneumonia. Int J Tuberc Lung Dis 2008; 12: pp. 1320-1326.
5. Reid M.J., Shah N.S.: Approaches to tuberculosis screening and diagnosis in people with HIV in resource-limited settings. Lancet Infect Dis 2009; 9: pp. 173-184.
6. Siddiqi K., Lambert M.L., Walley J.: Clinical diagnosis of smear-negative pulmonary tuberculosis in low-income countries: the current evidence. Lancet Infect Dis 2003; 3: pp. 288-296.
7. Mollura D.J., Azene E.M., Starikovsky A., et. al.: White Paper Report of the RAD-AID Conference on International Radiology for Developing Countries: identifying challenges, opportunities, and strategies for imaging services in the developing world. J Am Coll Radiol 2010; 7: pp. 495-500.
8. Panosian C., Coates T.J.: The new medical “missionaries”—grooming the next generation of global health workers. N Engl J Med 2006; 354: pp. 1771-1773.
9. AAMC.: 2003 Medical School Graduation Questionnaire.All Schools Report.2003.Association of American Medical CollegesWashington, DC:
10. Schultz S.H., Rousseau S.: International health training in family practice residency programs. Fam Med 1998; 30: pp. 29-33.
11. Thompson M.J., Huntington M.K., Hunt D.D., et. al.: Educational effects of international health electives on U.S. and Canadian medical students and residents: a literature review. Acad Med 2003; 78: pp. 342-347.
12. Dey C.C., Grabowski J.G., Gebreyes K., et. al.: Influence of international emergency medicine opportunities on residency program selection. Acad Emerg Med 2002; 9: pp. 679-683.
13. Nelson B.D., Lee A.C., Newby P.K., et. al.: Global health training in pediatric residency programs. Pediatrics 2008; 122: pp. 28-33.
14. Torjesen K., Mandalakas A., Kahn R., et. al.: International child health electives for pediatric residents. Arch Pediatr Adolesc Med 1999; 153: pp. 1297-1302.
15. Bazemore A.W., Henein M., Goldenhar L.M., et. al.: The effect of offering international health training opportunities on family medicine residency recruiting. Fam Med 2007; 39: pp. 255-260.
16. Federico S.G., Zachar P.A., Oravec C.M., et. al.: A successful international child health elective: the University of Colorado Department of Pediatrics’ experience. Arch Pediatr Adolesc Med 2006; 160: pp. 191-196.
17. Gupta A.R., Wells C.K., Horwitz R.I., et. al.: The International Health Program: the fifteen-year experience with Yale University’s Internal Medicine Residency Program. Am J Trop Med Hyg 1999; 61: pp. 1019-1023.
18. Miller W.C., Corey G.R., Lallinger G.J., et. al.: International health and internal medicine residency training: the Duke University experience. Am J Med 1995; 99: pp. 291-297.
19. Powell A.C., Mueller C., Kingham P., et. al.: International experience, electives, and volunteerism in surgical training: a survey of resident interest. J Am Coll Surg 2007; 205: pp. 162-168.
20. Keefer R.: Developing countries see clearly using donated imaging equipment. Am Coll Radiol Bull 2008; pp. 6-7.
21. Keefer R.: To the rescue. Am Coll Radiol Bull 2010; pp. 12-14.
22. Sawatsky A.P., Rosenman D.J., Merry S.P., et. al.: Eight years of the Mayo International Health Program: what an international elective adds to resident education. Mayo Clin Proc 2010; 85: pp. 734-741.
23. Crump J.A., Sugarman J.: Ethical considerations for short-term experiences by trainees in global health. JAMA 2008; 300: pp. 1456-1458.