
Rationale and Objectives
Little is known about the hemodynamics of gastrorenal shunt (GRS), a major drainage route of gastric fundal varices (FV), in patients with FV. The aim of this study was to clarify the hemodynamic features of GRS on Doppler sonography in relation to the grading and bleeding of FV.
Materials and Methods
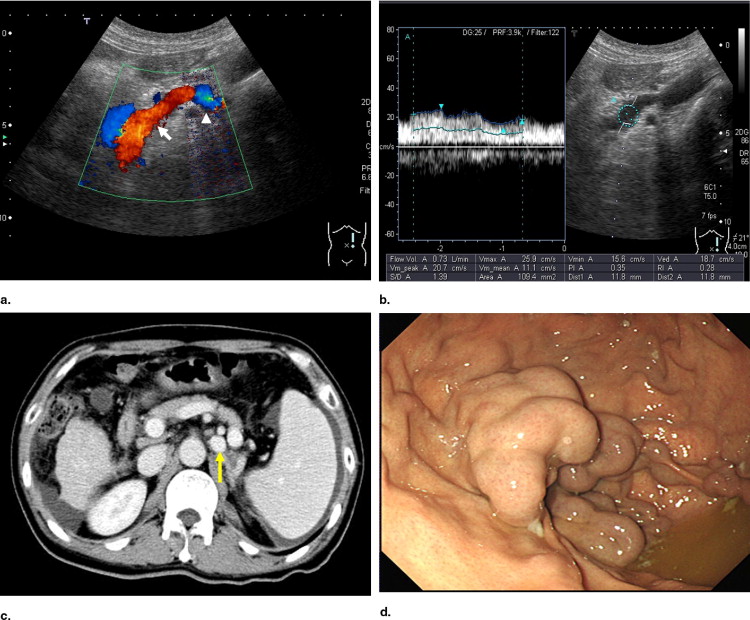
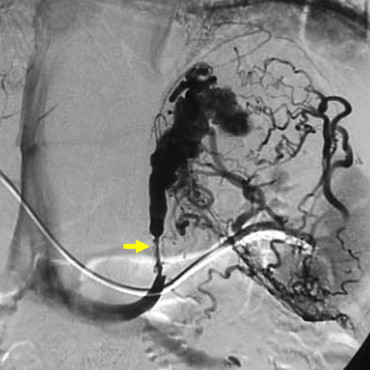
The study subjects consisted of 69 cirrhotic patients with FV. Diameter, flow velocity (FVe), and flow volume (FVo) of GRS were measured by Doppler ultrasound (US). The detection rate was compared to contrast-enhanced computed tomography (CECT), and percutaneous transhepatic portography (PTP) was used in six patients without GRS on CECT.
Results
The use of CECT detected GRS in 60 of 69 patients, and US, 58 of 69 patients. A false-negative result for detecting GRS on both CECT and US was found in one patient after PTP. The diameter, FVe, and FVo of GRS increased according to the endoscopic grade of FV: F1 (7.2 ± 1.3 mm, 9.8 ± 1.1 cm/s, 358.3 ± 123.4 ml/min), F2 (9.9 ± 3.3 mm, 12.8 ± 5.1 cm/s, 701.7 ± 411.3 ml/min), and F3 (11.8 ± 2.4 mm, 17.9 ± 8.3 cm/s, 1706.6 ± 989.5 ml/min). A significant difference was seen between F1 and F3 (diameter, P = .0022; FVe, P = .0133; FVo, P = .0007) and between F2 and F3 (FVe, P = .0112; FVo, P < .0001). FVe of GRS was significantly higher in bleeders (16.7 ± 8.1 cm/s) than in nonbleeders (12.2 ± 5.4 cm/s, P = .017), whereas the diameter and FVo were not significant.
Conclusion
Hemodynamics of GRS on Doppler sonograms reflected the grading and bleeding of FV. Doppler US may be valuable as a noninvasive method to evaluate the severity of FV.
Gastric fundal varices (FV) are known to be a considerable complication in patients with portal hypertension ( ). Although the rates of bleeding for FV have been reported to be lower than those for esophageal varices (EV), rupture from FV sometimes results in serious consequences in the clinical course ( ). Certain treatment methods using endoscopy, interventional techniques, and surgical procedures have been introduced for FV ( ). However, a few studies have reported risk factors for FV bleeding, and hemodynamic features associated with FV bleeding have not been clarified ( ).
There are a number of inflow vessels into FV: the left gastric, posterior gastric, and short gastric veins ( ). The main outflow pathway in the majority of FV is the gastrorenal shunt (GRS), and the blood flow manner of GRS may represent the clinical condition of FV. Watanabe et al. ( ), using the percutaneous transhepatic portography (PTP) technique, reported that the diameter of the GRS depended on the severity of FV. However, that study was based on a nonphysiologic condition using portal venous catheterization, and it lacked quantitative assessment. Little is known about the physiologic hemodynamic features of the GRS in patients with FV.
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Endoscopy
Get Radiology Tree app to read full this article<
Contrast-enhanced Computed Tomography
Get Radiology Tree app to read full this article<
Ultrasound
Equipment and settings
Get Radiology Tree app to read full this article<
Demonstration of gastrorenal shunt
Get Radiology Tree app to read full this article<
Percutaneous Transhepatic Portography
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Comparison of the Detection Rate of Gastrorenal Shunt Between Ultrasound and Contrast-enhanced Computed Tomography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Hemodynamic Features of Gastrorenal Shunt on the Sonograms
Get Radiology Tree app to read full this article<
![Figure 3, Color Doppler (72-year-old man with medium-grade gastric fundal varices [F2]). The sagittal plane of the color Doppler sonogram showed gastrorenal shunt with a to-and-fro appearance.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/HemodynamicFeaturesofGastrorenalShunt/2_1s20S1076633208001839.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Hemodynamics in the Gastrorenal Shunt (GRS) in Relation to the Grade of Gastric Fundal Varices
FV GRS (mean ± SD) Diameter (mm) FVe (cm/s) FVo (mL/m) F1 7.2 ± 1.3 ⁎ 9.8 ± 1.1 ‡ 358.3 ± 123.4 ⁎⁎ F2 9.9 ± 3.3 † 12.8 ± 5.1 § 701.7 ± 411.3 †† F3 11.8 ± 2.4 ⁎ † 17.9 ± 8.3 ‡ § 1706.6 ± 989.5 ⁎⁎ ††
FVe: flow velocity; FVo: flow volume.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Hemodynamics in the Gastrorenal Shunt (GRS) in Relation to the Bleeding of Gastric Fundal Varices
GRS (mean ± SD) Diameter (mm) FVe (cm/s) FVo (mL/m) Nonbleeder 10.2 ± 3.5 ⁎ 12.2 ± 5.4 † 843.8 ± 810.3 ‡ Bleeder 10.3 ± 2.5 ⁎ 16.7 ± 8.1 † 1187.1 ± 914.2 ‡
FVe: flow velocity; FVo: flow volume.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Sarin S.K., Lahoti D., Saxena S.P., et. al.: Prevalence, classification and natural history of gastric varices: A long-term follow-up study in 568 portal hypertension patients. Hepatology 1992; 16: pp. 1343-1349.
2. Bosch J., Abraldes J.G., Groszmann R.: Current management of portal hypertension. J Hepatol 2003; 38: pp. S54-S68.
3. Ryan B.M., Stockbrugger R.W., Ryan J.M.: A pathophysiologic, gastroenterologic, and radiologic approach to the management of gastric varices. Gastroenterology 2004; 126: pp. 1175-1189.
4. Lubel J.S., Angus P.W.: Modern management of portal hypertension. Intern Med J 2005; 35: pp. 45-49.
5. D’amico G., Pagliaro L., Bosch J.: The treatment of portal hypertension: A meta-analytic review. Hepatology 1995; 22: pp. 332-354.
6. Greenwald B.D., Caldwell S.H., Hespenheide E.E., et. al.: N -2-Butyl-cyanoacrylate for bleeding gastric varices: A United States pilot study and cost analysis. Am J Gastroenterol 2003; 98: pp. 1982-1988.
7. Tripathi D., Ferguson J.W., Therapondos G., et. al.: Review article: Recent advances in the management of bleeding gastric varices. Aliment Pharmacol Ther 2006; 24: pp. 1-17.
8. Kanagawa H., Mima S., Kouyama H., et. al.: Treatment of gastric fundal varices by balloon-occluded retrograde transvenous obliteration. J Gastroenterol Hepatol 1996; 11: pp. 51-58.
9. Koito K., Namieno T., Nagakawa T., et. al.: Balloon-occluded retrograde transvenous obliteration for gastric varices with gastrorenal or gastrocaval collaterals. AJR Am J Roentgenol 1996; 167: pp. 1317-1320.
10. Akahane T., Iwasaki T., Kobayashi N., et. al.: Changes in liver function parameters after occlusion of gastrorenal shunts with balloon-occluded retrograde transvenous obliteration. Am J Gastroenterol 1997; 92: pp. 1026-1030.
11. Yamagami T., Kato T., Iida S., et. al.: Change in the hemodynamics of the portal venous system after retrograde transvenous balloon occlusion of a gastrorenal shunt. AJR Am J Roentgenol 2003; 181: pp. 1011-1015.
12. Scott J., Dick R., Long R.G., et. al.: Percutaneous transhepatic obliteration of gastro-oesophageal varices. Lancet 1976; 2: pp. 53-55.
13. Sanyal A.J., Freedman A.M., Luketic V.A., et. al.: The natural history of portal hypertension after transjugular intrahepatic portosystemic shunts. Gastroenterology 1997; 112: pp. 889-898.
14. Chau T., Patch D., Chan Y., et. al.: “Salvage” transjugular intrahepatic portosystemic shunts: Gastric fundal compared with oesophageal variceal bleeding. Gastroenterology 1998; 114: pp. 981-987.
15. Barange K., Peron J.M., Imani K., et. al.: Transjugular intrahepatic portosystemic shunt in the treatment of refractory bleeding from ruptured gastric varices. Hepatology 1999; 30: pp. 1139-1143.
16. Tripathi D., Therapondos G., Jackson E., et. al.: The role of the transjugular intrahepatic portosystemic stent shunt (TIPSS) in the management of bleeding gastric varices: Clinical and haemodynamic correlations. Gut 2002; 51: pp. 270-274.
17. Boyer T.: Transjugular intrahepatic portosystemic shunt: Current status. Gastroenterology 2003; 124: pp. 1700-1710.
18. Thomas P.G., D’Cruz A.J.: Distal splenorenal shunting for bleeding gastric varices. Br J Surg 1994; 81: pp. 241-244.
19. Yamamoto J., Nagai M., Smith B., et. al.: Hand-assisted laparoscopic splenectomy and devascularization of the upper stomach in the management of gastric varices. World J Surg 2006; 30: pp. 1-6.
20. Kim T., Shijo H., Kokawa H., et. al.: Risk factors for hemorrhage from gastric fundal varices. Hepatology 1997; 25: pp. 307-312.
21. Akiyoshi N., Shijo H., Iida T., et. al.: The natural history and prognostic factors in patients with cirrhosis and gastric fundic varices without prior bleeding. Hepatol Res 2000; 17: pp. 145-155.
22. Matsumoto A., Kitamoto M., Imamura M., et. al.: Three-dimensional portography using multislice helical CT is clinically useful for management of gastric fundic varices. AJR Am J Roentgenol 2001; 176: pp. 899-905.
23. Ono N., Toyonaga A., Nishimura H., et. al.: Evaluation of magnetic resonance angiography on portosystemic collaterals in cirrhotic patients. Am J Gastroenterol 1997; 92: pp. 1515-1519.
24. Anderson C.M.: GI magnetic resonance angiography. Gastrointest Endosc 2002; 55: pp. S42-S48.
25. Watanabe K., Kimura K., Matsutani S., et. al.: Portal hemodynamics in patients with gastric varices: A study in 230 patients with esophageal and/or gastric varices using portal vein catheterization. Gastroenterology 1988; 95: pp. 434-440.
26. Kimura K., Ohto M., Matsutani S., et. al.: Relative frequencies of portosystemic pathways and renal shunt formation through the “posterior” gastric vein: Portographic study in 460 patients. Hepatology 1990; 12: pp. 725-728.
27. Grant E.G., Tessler F.N., Perrella R.R.: Clinical Doppler Imaging. AJR Am J Roentgenol 1989; 152: pp. 707-717.
28. Schmassmann A., Zuber M., Livers M., et. al.: Recurrent bleeding after variceal hemorrhage: Predictive value of portal venous duplex sonography. AJR Am J Roentgenol 1993; 160: pp. 41-47.
29. Ferrara K., Deangelis G.: Color flow mapping. Ultrasound Med Biol 1997; 23: pp. 321-345.
30. von Herbay A., Frieling T., Haeussinger D.: Color Doppler sonographic evaluation of spontaneous portosystemic shunts and inversion of portal venous flow in patients with cirrhosis. J Clin Ultrasound 2000; 28: pp. 332-339.
31. Yamada M., Ishida H., Komatsuda T., et. al.: Portal systemic shunt through the renal vein. Abdom Imaging 2006; 31: pp. 701-705.
32. Pugh R.N., Murray-Lyon I.M., Dawson J.L., et. al.: Transection of the esophagus for bleeding esophageal varices. Br J Surg 1973; 60: pp. 646-649.
33. The Japan Society for Portal Hypertension: The General Rules for Study of Portal Hypertension.2004.Kanehara & Co., LtdTokyo, Japan:pp. 37-50.
34. Kimura K., Tsuchiya Y., Ohto M., et. al.: Single-puncture method for percutaneous transhepatic portography using a thin needle. Radiology 1981; 139: pp. 748-749.
35. Takayasu K., Moriyama N., Shima Y., et. al.: Sonographic detection of large spontaneous spleno-renal shunts and its clinical significance. Br J Radiol 1984; 57: pp. 565-570.