
Rationale and Objectives
To evaluate the quality of stent lumen delineation using dual-source computed tomography (DSCT) in the standard-pitch mode (SP) as compared to the high-pitch mode (HP) in a phantom study.
Materials and Methods
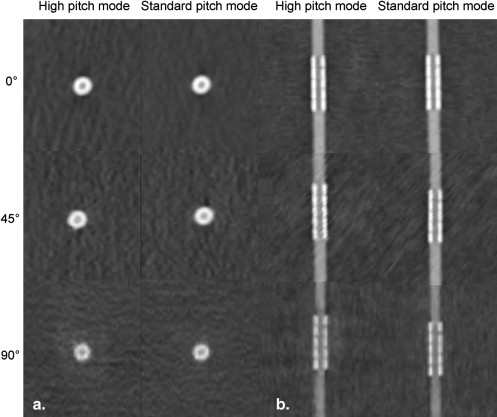
Forty different coronary stents placed in plastic tubes filled with contrast agent were imaged with a second generation DSCT system in a SP (pitch 0.23) and HP (pitch 3.4) mode in orientations of 0°, 45°, and 90° relative to the z-axis. Two observers independently measured the in-stent lumen and the attenuation values in the center of the stents. The artificial lumen narrowing (ALN) was calculated using the measured in-stent lumen and the nominal diameter of the plastic tube.
Results
Interobserver correlation was excellent for in-stent lumen (0.86) and attenuation measurements (0.91). There was no significant difference neither for ALN (SP: 54.7–62.8%; HP: 55.8–64.0%) nor attenuation (SP: 356–395 Hounsfield units [HU]; HP: 352–384 HU) between SP and HP mode. For both modes, the orientation of the stent relative to the z-axis significantly affected ALN and attenuation (each P < .001). CT volume dose index was significantly lower using HP mode as compared to SP mode ( P < .001).
Conclusion
The HP mode in DSCT provides visualization of the coronary in-stent lumen comparable to that measured in SP mode while reducing applied radiation dose in a stationary phantom model.
With a total of approximately 652,000 stent procedures performed in the United States in 2006, coronary artery stenting is the predominant procedure of nonsurgical myocardial revascularization . Although the introduction of drug-eluting stents into clinical practice significantly reduced in-stent restenosis rates compared with bare metal stents , in-stent restenosis and thrombosis remain the main problems of this frequent procedure with the restenosis rate still being 8.6–21.3% 1 year after treatment . Thus, early identification of in-stent restenosis is of clinical interest to avoid recurrent ischemic episodes, prevent myocardial infarction, and thereby improve long-term prognosis. Multidetector computed tomography (MDCT) has been shown to provide high diagnostic accuracy in the detection of coronary stenosis . However, evaluation of coronary stents with MDCT has remained difficult despite ongoing advances in CT technology. Although promising clinical results for stent assessment were reported for 64-slice MDCT ( ), evaluation of coronary stents with MDCT has remained difficult. Recently, the second generation of dual-source CT systems (DSCT) was introduced, providing high detector coverage with the use of two 128-section detectors. This DSCT allows CT coronary angiography (CTCA) at high-pitch (HP) values of up to 3.4 . The HP mode in combination with large detector coverage reduces acquisition time for CTCA to 0.25 seconds. The high diagnostic accuracy of CTCA in HP mode for the detection of coronary artery stenoses is maintained .
The purpose of our study was to evaluate and compare the quality of stent lumen delineation using DSCT in the standard-pitch mode (SP) as compared to the newly introduced HP mode.
Methods
Evaluated Stents and Experimental Setup
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Examined Stents
No. Name Manufacturer Material Coating Diameter
(mm) Length
(mm) Strut Thickness
(mm) 1 CCSV Micro Science Medical Stainless steel 316L Tantalum 3 16 0.6–0.8 2 Coroflex B. Braun Stainless steel 316L — 3 25 0.100 3 Coroflex Blue B. Braun Cobalt-chromium alloy (L605) — 2.5 16 0.065 4 Coroflex Delta B. Braun Stainless steel 316L — 3.5 16 0.120 5 Crossflex Cordis Stainless steel 316L — 3 22 0.152 6 CSG (R010F26) Abbott Vascular Devices Stainless steel 316L — 3 24 0.3 7 Cypher Cordis Stainless steel 316L — 3 13 0.14 8 Duett Guidant Stainless steel 316L — 3 7 0.14 9 Express 2 Boston Scientific Stainless steel 316L — 4 20 0.13 10 F1 Large (010FF12) Abbott Vascular Devices Stainless steel 316L — 3 12 0.09 11 Flex AS Phytis Stainless steel 316L DLC 3 7 0.09 12 Jograft Abbott Vascular Devices Stainless steel 316L + PTFE-graft — 3 9 0.091–0.124 13 Lekton Biotronik Stainless steel 316L Silicon-carbide 2.75 15 0.8–1.0 14 Magic Wallstent Boston Scientific Elgiloy — 4 32 0.1 15 Mansfield Coronary Stent Mansfield Tantalum — 3.5 20 0.1 16 NIR Royal Boston Scientific Stainless steel 316LS Gold 3 25 0.14 17 Radius Boston Scientific Nitinol — 3 20 0.08–0.09 18 Symbiot Boston Scientific Nitinol — 4 20 0.110 19 Tantal Abbott Vascular Devices Tantalum based alloy — 3 5 0.08 20 Tantal Sandwich Abbott Vascular Devices 316L (inside), Ta (intermediate), 316L (outside) — 3 18 0.07 21 Vision Guidant Cobalt-chromium alloy — 3 15 0.81 22 Endeavor Medtronic Cobalt-chromium alloy Phosphorylcholine + ABT578 3 30 0.091 23 Coroflex Theca Braun Stainless steel 316L PTFEP-Polyzene-F 3 16 0.12 24 STCC Eucatech Cobalt-chromium alloy — 3 18 0.066 25 Coroflex Please Braun Stainless Steel 316L Polysulfone + Paclitaxel 3 19 0 26 Chrono Sorin Biomedica Cobalt-chromium alloy Carbofilm 3 20 0.08 27 CoStar Biotronik Cobalt-chromium alloy Paclitaxel/PLGA 3 16 0.09 28 Invastent Volo Krauth CardioVascular Stainless steel 316L — 3 27 0,08/0,1 29 STS Flex Eucatech Stainless steel 316L — 3 18 0,085–0,13 30 Yukon Plus Translumina Stainless steel 316L Diamond-like carbon rainbow coated 3 25 0.097 at 2.5mm 31 Yukon Choice Translumina Stainless steel 316L By choice 3 21 0.09 32 PRO Kinetic Biotronik Cobalt-chromium alloy PROBIO, SiC 3 15 0.06 33 Camouflage (CFL) Eucatech Stainless steel 316L Polysaccharide 3 18 0.1 34 Twin-Rail Krauth CardioVascular Stainless steel 316L — 3/1,5 15 0.1 35 Bx Velocity Cordis/J&J Stainless steel 316L — 4.5 18 0.14 36 Apolo Bionert Iberhospitex Stainless steel 316L, treated with O2 ion jets — 3 14 0.115 37 BiodivYsio OC Abbott Vascular Devices Stainless steel 316L Dexamethasone on phosphorylcholine 3 22 0.091 38 ZoMaxx Abbott Vascular Devices Stainless steel 316L/Tantalum — 3 15 0.074 39 Tantal Coronary 58 μm Abbott Vascular Devices/Guidant Tantalum — 3 19 0.58 40 Pura AS16 Devon Medical Stainless steel 316L — 2.5–3.5 16 0.08
Get Radiology Tree app to read full this article<
Acquisition Parameters
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose Parameters
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Interobserver Variability
Get Radiology Tree app to read full this article<
![Figure 3, Bland-Altman analysis comparing measurements from standard-pitch mode and high-pitch mode concerning attenuation (a) and in-stent lumen diameter (b) of coronary stents. Lines represent mean of results and limits of agreement (mean ± 1.96 standard deviation [SD]). HU, Hounsfield units.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/HighPitch128SliceDualSourceCTfortheAssessmentofCoronaryStentsinaPhantomModel/2_1s20S1076633210003478.jpg)
Get Radiology Tree app to read full this article<
In-stent Lumen Diameters
Get Radiology Tree app to read full this article<
Table 2
In-stent Lumen Diameter (Abs) and Artificial Lumen Narrowing (ALN) in Standard-pitch and High-pitch Mode Measured from Images Reconstructed with the B46f kernel at Three Different Orientations of the Stent
Reader 1 Reader 2 0° ∗ 45° ∗ 90° ∗ 0° ∗ 45° ∗ 90° ∗ Abs (mm) ALN (%) Abs (mm) ALN (%) Abs (mm) ALN (%) Abs (mm) ALN (%) Abs (mm) ALN (%) Abs (mm) ALN (%) Standard-pitch mode 1.1 ± 0.31 62.8 ± 10.5 1.1 ± 0.31 61.8 ± 10.7 1.1 ± 0.26 62.1 ± 8.6 1.2 ± 0.26 60.4 ± 8.6 1.3 ± 0.31 58.3 ± 10.4 1.4 ± 0.27 54.7 ± 8.9 High-pitch mode 1.1 ± 0.22 64.0 ± 9.0 1.1 ± 0.0.25 61.7 ± 10.8 1.1 ± 0.29 62.7 ± 9.7 1.1 ± 0.23 63.8 ± 7.9 1.3 ± 0.30 56.1 ± 9.7 1.3 ± 0.33 55.8 ± 11.1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Attenuation of the Stent Lumen
Get Radiology Tree app to read full this article<
Table 3
Mean Attenuation of the Stent Lumen (Hounsfield units [HU]) and Difference between Attenuation within the Stent Lumen and the Unstented Segment of the Vessel Phantom (ΔHU) in Standard-pitch Mode and High-pitch Mode Measured from Images Reconstructed with the B46f kernel at Three Different Orientations of the Stent
Reader 1 Reader 2 0° ∗ 45° ∗ 90° ∗ 0° ∗ 45° ∗ 90° ∗ HU (ΔHU) HU (ΔHU) HU (ΔHU) HU (ΔHU) HU (ΔHU) HU (ΔHU) Standard-pitch mode 395.0 ± 69.3 56.3 ± 64.9 412.5 ± 98.6 114.5 ± 100.8 356.6 ± 106.3 163.1 ± 83.9 356.2 ± 85.2 23.3 ± 59.9 381.3 ± 92.3 93.0 ± 96.0 353.4 ± 100.8 151.3 ± 103.0 High-pitch mode 384.3 ± 51.0 42.6 ± 47.5 419.6 ± 93.0 123.9 ± 97.9 377.1 ± 125.8 177.4 ± 105.0 352.2 ± 63.0 13.7 ± 62.1 393.8 ± 86.7 97.6 ± 86.8 371.2 ± 133.1 166.2 ± 126.1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Mean Artificial Lumen Narrowing (ALN) and ΔHU of Examined Stents at 0°
ALN [%] ΔHU No. Name SP HP SP HP 1 CCSV 45.5 51.0 82.0 98.7 2 Coroflex 59.7 60.7 33.9 76.8 3 Coroflex Blue 54.3 55.2 18.1 −23.3 4 Coroflex Delta 61.0 63.2 26.8 30.9 5 Crossflex 63.8 67.8 80.5 62.6 6 CSG (R010F26) 64.8 63.8 35.9 63.5 7 Cypher 59.0 58.5 25.5 39.0 8 Duett 68.3 69.7 59.5 56.1 9 Express 2 69.7 72.7 94.4 99.1 10 F1 Large (010FF12) 56.0 61.2 38.2 13.1 11 Flex AS 58.0 62.2 37.0 39.1 12 Jograft 71.7 70.5 58.0 65.9 13 Lekton 60.8 64.5 32.0 36.9 14 Magic Wallstent 71.0 71.7 −114.4 −93.1 15 Mansfield Coronary Stent 86.7 83.0 284.7 144.3 16 NIR Royal 71.2 72.0 32.4 14.0 17 Radius 46.5 52.7 28.2 3.4 18 Symbiot 51.2 55.2 5.7 11.2 19 Tantal 81.3 83.0 22.1 46.1 20 Tantal Sandwich 65.2 66.8 93.9 67.9 21 Vision 67.0 70.7 96.5 103.8 22 Endeavor 52.7 56.3 41.0 34.0 23 Coroflex Theca 56.7 61.5 −3.7 23.3 24 STCC 58.2 60.8 6.3 3.8 25 Coroflex Please 58.8 65.3 16.6 −31.1 26 Chrono 57.8 61.5 11.5 24.6 27 CoStar 61.8 64.0 56.5 −7.3 28 Invastent Volo 50.8 56.8 24.6 4.5 29 STS Flex 52.5 56.7 −2.8 1.7 30 Yukon Plus 58.8 62.7 53.6 16.3 31 Yukon Choice 57.0 56.8 20.9 −8.5 32 PRO Kinetic 57.2 59.8 13.5 4.1 33 Camouflage (CFL) 58.7 58.2 21.0 30.6 34 Twin-Rail 71.2 70.7 −7.0 19.3 35 Bx Velocity 67.7 68.8 76.6 77.5 36 Apolo Bionert 55.5 56.5 −2.5 −24.0 37 BiodivYsio OC 57.0 54.7 33.2 36.9 38 ZoMaxx 67.5 72.7 78.4 −19.5 39 Tantal Coronary 58μm 79.3 80.2 90.7 −23.8 40 Pura AS16 53.2 55.7 −7.2 6.9
ALN, artificial lumen narrowing; ΔHU, difference of the attenuation between unstented and stented vessel lumen; SP, standard-pitch mode; HP, high-pitch mode.
Get Radiology Tree app to read full this article<
Image Noise
Get Radiology Tree app to read full this article<
Radiation Dose Parameters
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Lloyd-Jones D., Adams R., Carnethon M., et. al.: Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2009; 119: pp. e21-e181.
2. Moses J.W., Leon M.B., Popma J.J., et. al.: Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003; 349: pp. 1315-1323.
3. Stone G.W., Ellis S.G., Cox D.A., et. al.: A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med 2004; 350: pp. 221-231.
4. Menichelli M., Parma A., Pucci E., et. al.: Randomized trial of Sirolimus-Eluting Stent Versus Bare-Metal Stent in Acute Myocardial Infarction (SESAMI). J Am Coll Cardiol 2007; 49: pp. 1924-1930.
5. Stone G.W., Ellis S.G., Cannon L., et. al.: Comparison of a polymer-based paclitaxel-eluting stent with a bare metal stent in patients with complex coronary artery disease: a randomized controlled trial. JAMA 2005; 294: pp. 1215-1223.
6. Leschka S., Alkadhi H., Plass A., et. al.: Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 2005; 26: pp. 1482-1487.
7. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
8. Das K.M., El-Menyar A.A., Salam A.M., et. al.: Contrast-enhanced 64-section coronary multidetector CT angiography versus conventional coronary angiography for stent assessment. Radiology 2007; 245: pp. 424-432.
9. Oncel D., Oncel G., Karaca M.: Coronary stent patency and in-stent restenosis: determination with 64-section multidetector CT coronary angiography—initial experience. Radiology 2007; 242: pp. 403-409.
10. Schuijf J.D., Pundziute G., Jukema J.W., et. al.: Evaluation of patients with previous coronary stent implantation with 64-section CT. Radiology 2007; 245: pp. 416-423.
11. Van Mieghem C.A., Cademartiri F., Mollet N.R., et. al.: Multislice spiral computed tomography for the evaluation of stent patency after left main coronary artery stenting: a comparison with conventional coronary angiography and intravascular ultrasound. Circulation 2006; 114: pp. 645-653.
12. Achenbach S., Marwan M., Schepis T., et. al.: High-pitch spiral acquisition: a new scan mode for coronary CT angiography. J Cardiovasc Comput Tomogr 2009; 3: pp. 117-121.
13. Leschka S., Stolzmann P., Desbiolles L., et. al.: Diagnostic accuracy of high-pitch dual-source CT for the assessment of coronary stenoses: first experience. Eur Radiol 2009; 19: pp. 2896-2903.
14. Maintz D., Burg M.C., Seifarth H., et. al.: Update on multidetector coronary CT angiography of coronary stents: in vitro evaluation of 29 different stent types with dual-source CT. Eur Radiol 2009; 19: pp. 42-49.
15. Maintz D., Seifarth H., Raupach R., et. al.: 64-slice multidetector coronary CT angiography: in vitro evaluation of 68 different stents. Eur Radiol 2006; 16: pp. 818-826.
16. Seifarth H., Ozgun M., Raupach R., et. al.: 64- versus 16-slice CT angiography for coronary artery stent assessment: in vitro experience. Invest Radiol 2006; 41: pp. 22-27.
17. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
18. Achenbach S., Marwan M., Ropers D., et. al.: Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010; 31: pp. 340-346.
19. Haraldsdottir S., Gudnason T., Sigurdsson A.F., et. al.: Diagnostic accuracy of 64-slice multidetector CT for detection of in-stent restenosis in an unselected, consecutive patient population. Eur J Radiol 2009; Jun 29 [Epub ahead of print]
20. Sun Z., Almutairi A.M.: Diagnostic accuracy of 64 multislice CT angiography in the assessment of coronary in-stent restenosis: a meta-analysis. Eur J Radiol 2010; 73: pp. 266-273.
21. Oncel D., Oncel G., Tastan A., et. al.: Evaluation of coronary stent patency and in-stent restenosis with dual-source CT coronary angiography without heart rate control. AJR Am J Roentgenol 2008; 191: pp. 56-63.