
Rationale and Objectives
The purpose of this study was to illustrate the imaging findings on high-resolution 3T magnetic resonance neurography (MRN) in patients with suprascapular nerve (SSN) neuropathy.
Materials and Methods
From 3T MRN examinations performed for brachial plexus evaluation in 51 patients over a 3-year period, 15 patients with final diagnosis of suprascapular neuropathy were recruited. The diagnosis was confirmed by electrodiagnostic studies (EDS), clinical, and/or surgical follow-up examinations. Studies performed for the evaluation of tumor, neurofibromatosis, or known diffuse polyneuropathy were excluded.
Results
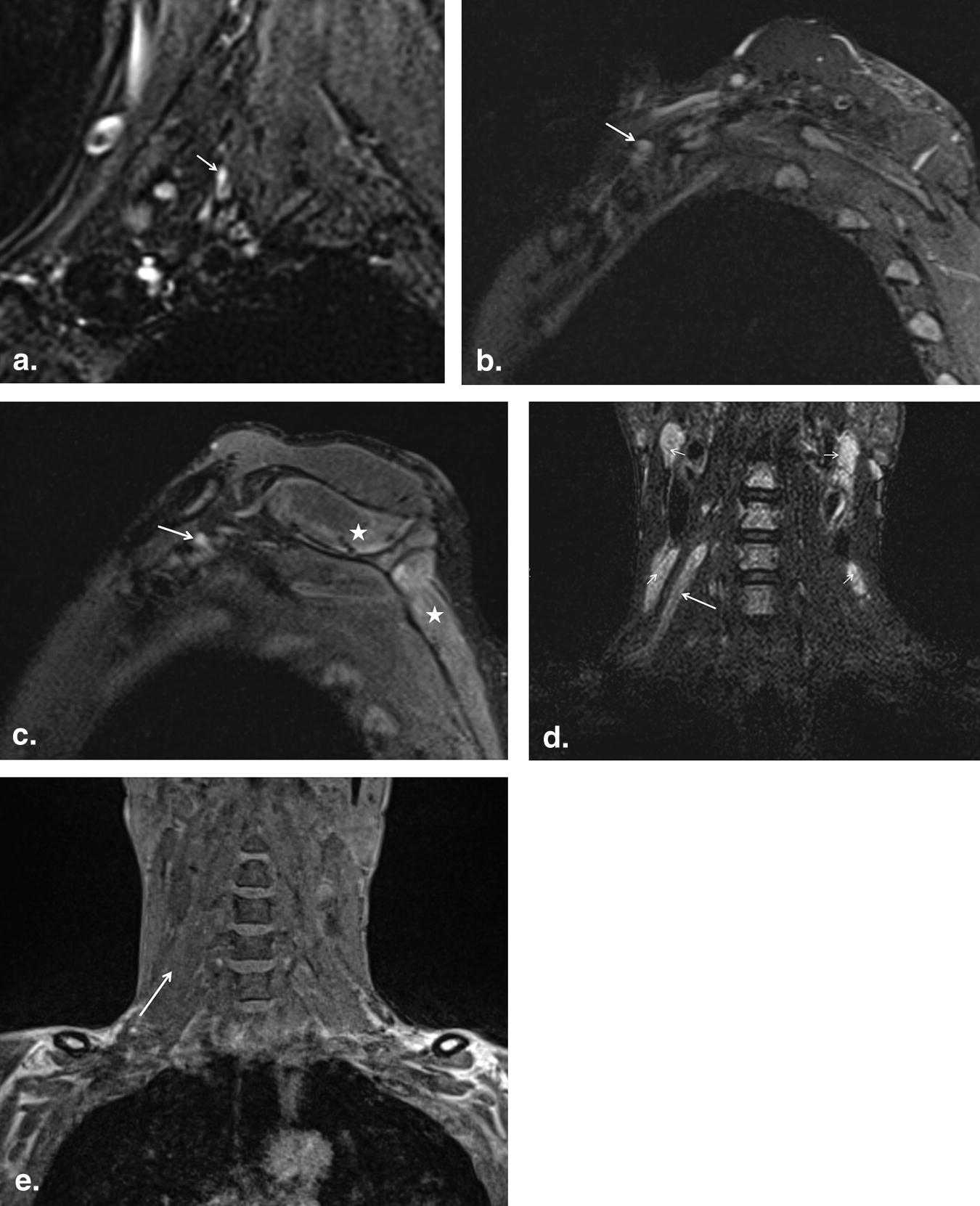
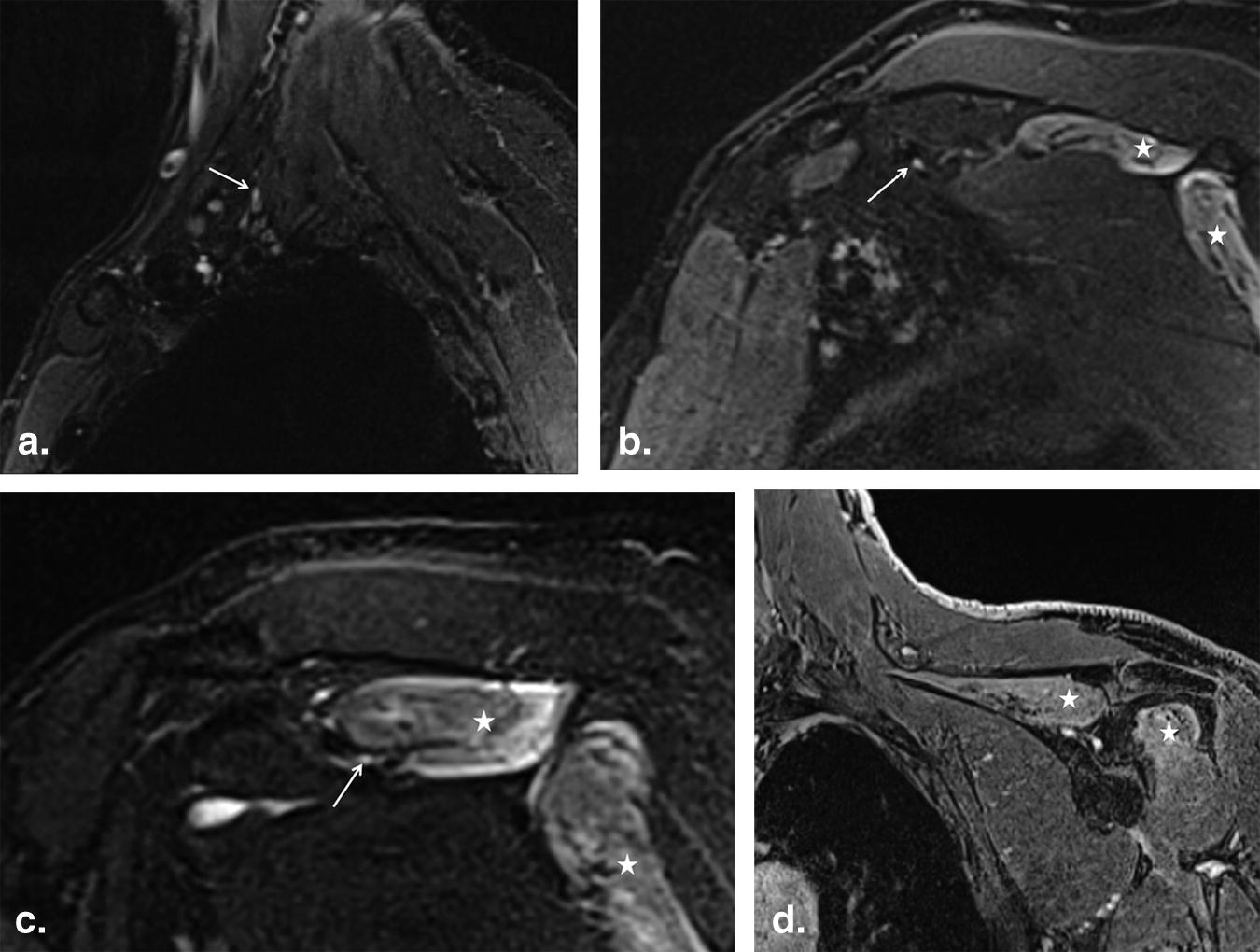
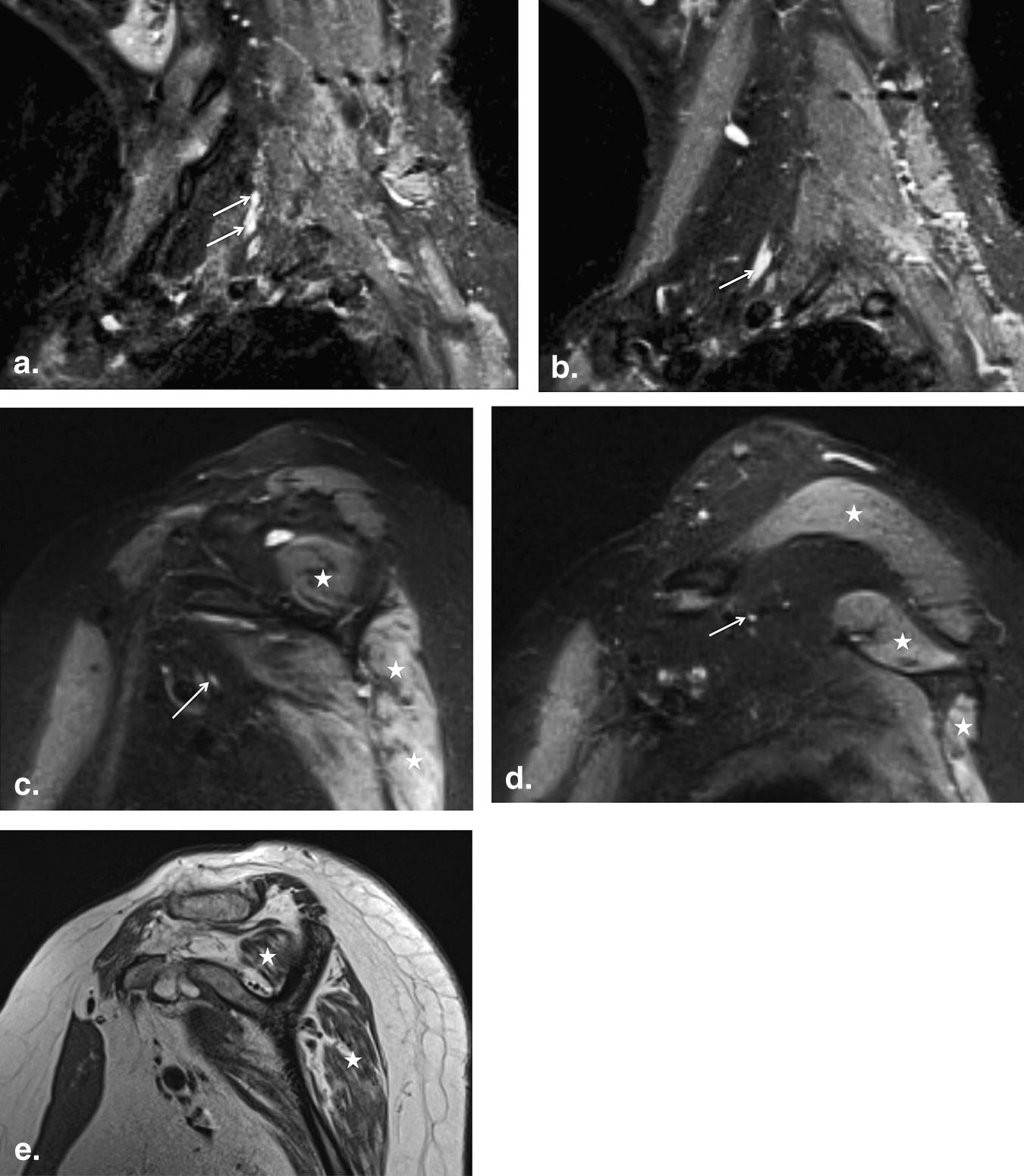
Two cases were excluded due to suboptimal imaging related to motion degradation and poor signal-to-noise ratio. MRN depicted asymmetric enlargement and/or abnormal T2 hyperintensity of C5 nerve root (10/13 cases), C6 nerve root (10/13 cases), both C5 and C6 nerve roots (7/13 cases), upper trunk (11/13 cases) and SSN (11/13 cases), and other brachial plexus segments involvement (4/13 cases). MR findings of denervation changes in the ipsilateral supraspinatus and infraspinatus muscles were detected in 12/13 cases. In all seven cases where contrast-enhanced images were available, MRN demonstrated enhancement of the denervated muscles but did not provide any additional information regarding the nerve abnormality. None of the MRN studies revealed a mass lesion along the course of the SSN.
Conclusion
3T MRN is a valuable diagnostic tool in clinically suspected cases of suprascapular neuropathy, because it can directly demonstrate the nerve abnormality, as well as secondary muscle denervation changes. The reader should be aware that brachial plexopathy may coexist in patients with clinical diagnosis of SSN neuropathy.
Suprascapular neuropathy constitutes a relatively uncommon, yet frequently overlooked cause of shoulder pain and weakness, which usually affects athletes and young individuals . Because of its superficial location, long course, and close anatomic relationship to rigid structures, the suprascapular nerve (SSN) is at increased risk for injury and entrapment ( Fig 1 ). In cases of trauma, the SSN is more commonly affected in areas where nerve mobility is limited, such as the suprascapular and spinoglenoid notches . However, a less well-described, though potentially important site of traumatic involvement of the SSN is at the level of the brachial plexus, where inflammation, stretching, or tear of the plexus may occur, potentially leading to upper extremity pain and dysfunction .
 Open full size image
Open full size image
Figure 1
Illustration demonstrates the supraclavicular course of the suprascapular nerve as it courses through the suprascapular notch and the spinoglenoid notch.
Get Radiology Tree app to read full this article<
Subjects and methods
Get Radiology Tree app to read full this article<
Table 1
3T MR Protocol for Brachial Plexus Neurography Employed in the Study
MR Sequence FOV Slice Thickness TR/TE Matrix T1 coronal 30 4.0 881/11 512 × 512 STIR coronal SPACE 30 1.0 1500/97 256 × 256 T2 SPACE sagittal 25 1.0 1000/97 256 × 256 T1 sagittal affected side 22–24 3.0 804/8 384 × 384 STIR sagittal affected side 22–24 3.0 5210/18 256 × 256 Contrast optional T1 coronal fs VIBE prebilateral 30 0.7 4.19/1.66 384 × 384 0.1 mmol/kg, 2 mL/second T1 coronal fs VIBE postbilateral 30 0.7 4.19/1.66 384 × 384
fs, fat suppressed; FOV, field of view; STIR, short tau inversion recovery; VIBE, volume interpolated breath-hold examination; SPACE, sampling perfection with application optimized contrast with varying flip angles; TR, repetition time; TE, echo time.
TR and TE are presented in ms; slice thickness in mm; FOV in cm.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Clinical, Demographic, EDS, and MRN Findings of Patients with SSN Neuropathy
Case Gender/Age (y) History Physical Examination Findings EDS Findings MRN Findings Other Findings Surgical Findings Final Diagnosis Outcome 1 M/56 Rt shoulder pain, CLL, hepatitis C, recent VZV infection Rt upper extremity weakness (3/5), muscle wasting, limitation in ROM, vesicular rash over Rt shoulder Not performed C3-6 myelitis, neuropathy of the Lt C5 nerve root, upper trunk and SSN. Mild subacute denervation changes of supra- and infraspinatus muscles C3-C6 myelitis Not performed VZV SSN neuritis and myelitis Symptoms resolved after 1–2 weeks of acyclovir treatment 2 M/55 Lt lateral shoulder weakness and pain for 5-months’ radiating anteriorly and posteriorly 3/5 weakness, especially in external rotation along with muscle wasting around the shoulder SSN neuropathy Neuropathy of the Lt C5 nerve root, upper trunk and SSN. Mild subacute denervation changes in supra- and infraspinatus muscles None No mass lesion or nerve inflammation Isolated SSN neuropathy Patient reported resolution of symptoms on a 3-month follow-up 3 M/49 Lt shoulder pain and weakness. History of MVA 9-months ago Supraspinatus muscle atrophy. 3/5 weakness in shoulder abduction SSN injury Neuroma of the Lt C6 nerve root, upper trunk and SSN. Subacute denervation changes of supra- and infraspinatus muscles Small Lt C5-C6 foraminal disc protrusion Not performed Lt C6 neuroma in continuity and posttraumatic SSN neuropathy Managed conservatively and reported gradual resolution of symptoms on a 6-week follow-up 4 F/65 Lt shoulder pain and weakness. History of MVA 11 months ago Multifocal muscle weakness and atrophy. Limitation in ROM in all directions Lt C5 nerve root avulsion, upper trunk neuropathy Neuropathy of the Lt C5, C6 nerve roots, upper trunk and SSN. Late subacute denervation changes in multiple muscles Multilevel moderate cervical spondylosis MRN findings confirmed. Neurolysis was performed Post traumatic brachial plexopathy, SSN and axillary neuropathy Significant resolution of symptoms after surgery 5 F/65 Sudden onset of Rt shoulder pain and weakness 3/5 weakness in the right upper extremity. Limitation in ROM Rt C5 radiculopathy Neuropathy of the Rt C5, C6 nerve roots, upper trunk and SSN. Subacute denervation changes in multiple muscles Mild-moderate multilevel cervical spondylosis Not performed Acute idiopathic brachial plexopathy, SSN and axillary neuropathy Managed conservatively and significant improvement was reported on a 4-month follow-up 6 F/40 Recent onset Rt upper extremity weakness and numbness. History of rheumatoid arthritis, mononeuritis multiplex, and hypothyroidism 3/5 weakness in the Rt upper extremity. Diminished light touch, pinprick and temperature sensation on dorsal surface of right forearm and deltoid Rt upper trunk brachial plexopathy Rt C6, C7, C8 and T1 nerve roots, trunks, cords and SSN hyperintensity and enlargement. Mild subacute denervation changes of supra- and infraspinatus muscles Cervical spondylosis Not performed Cervical spondylosis Managed conservatively and subsequently lost to follow-up 7 M/48 Lt upper extremity weakness and numbness 4 months after a posterior cervical spine decompression and fusion surgery Atrophy and weakness in the Lt supra-, infraspinatus, deltoid, biceps, and triceps muscles. Limitation in ROM. Severe injury to the left upper trunk of the brachial plexus Hyperintensity of the Lt C5, C6 nerve roots, upper trunk, SSN, axillary, and radial nerves. Denervation changes of supra- and infraspinatus muscles None Not performed Stretch Injury Managed with physical therapy with improvement 8 M/60 History of trauma to the Rt shoulder presented with pain and weakness 3/5 weakness in the Rt upper extremity with some limitation in ROM Not performed Moderate hyperintensity in C6. Mild fatty infiltration and edema in supra- and infraspinatus muscles. Multilevel cervical spondylosis with mild central canal stenosis Not performed Stretch injury Some improvement on follow-ups 9 M/26 History of hemophilia and Rt shoulder synovectomy. Rt upper extremity pain and weakness 4/5 weakness in the Rt triceps muscle. Decreased pinprick over right lateral shoulder and arm as well as the dorsum of the hand. Mild Rt SSN injury Moderate hyperintensity in C5, C6, and upper trunk. No denervation change in the muscles. None Not performed Idiopathic Symptoms worsened on 4-month follow-up 10 M/53 Recurrent desmoid tumors. Five surgeries in the Rt axilla, chest region, and 2 courses of radiotherapy presented with pain, weakness and numbness in the Rt arm Severe weakness of the entire Rt arm muscles along with decreased pinprick in fingers. Marked limitation in all ROM Rt-sided diffuse brachial plexopathy Rt-sided neuropathy of all the nerve roots, trunks and nerves including SSN. Diffuse enhancement of muscles. No atrophy. Mild edema of supra-and infraspinatus muscles. Disc herniation at the C5-C6 level Not performed Radiation-induced plexopathy No improvement on 6 month follow-up 11 M/51 Sudden severe bilateral arm weakness along with pain in the shoulders and neck area 3/5 weakness in both proximal upper extremities with normal sense and limitation in ROM Multifocal changes in a patchy distribution in C5-C8
myotomes Moderate hyperintensity of C5, C6, upper trunk, and SSN with mild enlargement of C6. Mild edema and fatty infiltration supra- and infraspinatus muscles. None Not performed Brachial plexitis Significant improvement on a 9-month follow-up 12 M/44 Severe pain and weakness on the Rt shoulder Marked weakness of supra- and infraspinatus, biceps, and deltoid muscles along with marked limitation in ROM Severe denervation in the Rt deltoid
and biceps with lesser degrees of denervation in scattered Rt upper limb muscles Neuropathy of C5 with mild hyperintensity of SSN. Moderate atrophy, edema and fatty infiltration of supra and infraspinatus muscles. Severe cervical spinal stenosis Neurolysis and nerve graft was performed Brachial plexitis Some improvement was reported after surgery 13 M/74 Progressive pain and weakness on shoulders bilaterally after fall 2–3/5 weakness of supra- and infraspinatus, and deltoid muscles with limitations in ROM Diffuse cervical radiculopathy versus brachial plexopathy Hyperintensity and enlargement of bilateral C5-C7 nerve roots, worse of C6, upper and middle trunks and their divisions including SSN. Mild atrophy and edema of supra- and infraspinatus muscles. Spondylolisthesis and disc desiccation of C4 on C5 and
C6 on C7.
Developmental central canal stenosis. Not performed Stretch injury No further follow-up
CLL, chronic lymphocytic leukemia; EDS, electrodiagnostic studies; F, female; Lt, left; M, male; MRN, magnetic resonance neurography; MVA, motor vehicle accident; ROM, range of motion (abduction and external rotation); Rt, right; SSN, suprascapular nerve; VZV, varicella zoster virus.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ludig T., Walter F., Chapuis D., et. al.: MR imaging evaluation of suprascapular nerve entrapment. Eur Radiol 2001; 11: pp. 2161-2169.
2. Padua L., LoMonaco M., Padua R., et. al.: Suprascapular nerve entrapment. Neurophysiological localization in 6 cases. Acta Orthop Scand 1996; 67: pp. 482-484.
3. Duparc F., Coquerel D., Ozeel J., et. al.: Anatomical basis of the suprascapular nerve entrapment, and clinical relevance of the supraspinatus fascia. Surg Radiol Anat 2010; 32: pp. 277-284.
4. Sureka J., Cherian R.A., Alexander M., et. al.: MRI of brachial plexopathies. Clin Radiol 2009; 64: pp. 208-218.
5. Piasecki D.P., Romeo A.A., Bach B.R., et. al.: Suprascapular neuropathy. J Am Acad Orthop Surg 2009; 17: pp. 665-676.
6. Gosk J., Urban M., Rutowski R.: Entrapment of the suprascapular nerve: anatomy, etiology, diagnosis, treatment. Orthop Traumatol Rehabil 2007; 9: pp. 68-74.
7. Walsworth M.K., Mills J.T., Michener L.A.: Diagnosing suprascapular neuropathy in patients with shoulder dysfunction: a report of 5 cases. Phys Ther 2004; 84: pp. 359-372.
8. Lee B.C., Yegappan M., Thiagarajan P.: Suprascapular nerve neuropathy secondary to spinoglenoid notch ganglion cyst: case reports and review of literature. Ann Acad Med Singapore 2007; 36: pp. 1032-1035.
9. Romeo A.A., Rotenberg D.D., Bach B.R.: Suprascapular neuropathy. J Am Acad Orthop Surg 1999; 7: pp. 358-367.
10. Solheim L.F., Roaas A.: Compression of the suprascapular nerve after fracture of the scapular notch. Acta Orthop Scand 1978; 49: pp. 338-340.
11. Carroll K.W., Helms C.A., Otte M.T., et. al.: Enlarged spinoglenoid notch veins causing suprascapular nerve compression. Skeletal Radiol 2003; 32: pp. 72-77.
12. Ferretti A., Cerullo G., Russo G.: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987; 69: pp. 260-263.
13. Wainner R.S., Fritz J.M., Irrgang J.J., et. al.: Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine 2003; 28: pp. 52-62.
14. Lauder T.D., Dillingham T.R., Andary M., et. al.: Predicting electrodiagnostic outcome in patients with upper limb symptoms: are the history and physical examination helpful?. Arch Phys Med Rehabil 2000; 81: pp. 436-441.
15. Ringel S.P., Treihaft M., Carry M., et. al.: Suprascapular neuropathy in pitchers. Am J Sports Med 1990; 18: pp. 80-86.
16. Jablecki C.K., Andary M.T., So Y.T., et. al.: Literature review of the usefulness of nerve conduction studies and electromyography for the evaluation of patients with carpal tunnel syndrome. AAEM Quality Assurance Committee. Muscle Nerve 1993; 16: pp. 1392-1414.
17. Sallomi D., Janzen D.L., Munk P.L., et. al.: Muscle denervation patterns in upper limb nerve injuries: MR imaging findings and anatomic basis. AJR Am J Roentgenol 1998; 171: pp. 779-784.
18. Hazrati Y., Miller S., Moore S., et. al.: Suprascapular nerve entrapment secondary to a lipoma. Clin Orthop Relat Res 2003; 411: pp. 124-128.
19. Fritz R.C., Helms C.A., Steinbach L.S., et. al.: Suprascapular nerve entrapment: evaluation with MR imaging. Radiology 1992; 182: pp. 437-444.
20. Zhang Z., Song L., Meng Q., et. al.: Morphological analysis in patients with sciatica: a magnetic resonance imaging study using three-dimensional high-resolution diffusion-weighted magnetic resonance neurography techniques. Spine 2009; 34: pp. 245-250.
21. Chhabra A., Williams E.H., Wang K.C., et. al.: MR neurography of neuromas related to nerve injury and entrapment with surgical correlation. AJNR Am J Neuroradiol 2010 Feb 4; [Epub ahead of print]
22. Filler A.G., Haynes J., Jordan S.E., et. al.: Sciatica of nondisc origin and piriformis syndrome: diagnosis by magnetic resonance neurography and interventional magnetic resonance imaging with outcome study of resulting treatment. J Neurosurg Spine 2005; 2: pp. 99-115.
23. Du R., Auguste K.I., Chin C.T., et. al.: Magnetic resonance neurography for the evaluation of peripheral nerve, brachial plexus, and nerve root disorders. J Neurosurg 2010; 112: pp. 362-371.
24. Zhou L., Yousem D.M., Chaudhry V.: Role of magnetic resonance neurography in brachial plexus lesions. Muscle Nerve 2004; 30: pp. 305-309.
25. Van Es H.W., Bollen T.L., van Heesewijk H.P.: MRI of the brachial plexus: a pictorial review. Eur J Radiol 2010; 74: pp. 391-402.