
Rationale and Objectives
Nocardiosis is difficult to diagnose, and the diagnosis is thus frequently delayed. High-resolution computed tomography (HRCT) findings of patients with pulmonary nocardiosis have been documented in few reports. Our study objective was to assess HRCT findings of patients with pulmonary nocardiosis.
Materials and Methods
This was a retrospective study of 20 consecutive patients with pulmonary Nocardia infections who underwent HRCT of the chest at our institutions from January 2011 to August 2014. After the exclusion of two patients with concurrent infections, the study group comprised 18 patients (11 men, 7 women; age range, 39–83 years; mean, 67.9 years) with pulmonary Nocardia infections. Parenchymal abnormalities, enlarged lymph nodes, and pleural effusion were evaluated on HRCT.
Results
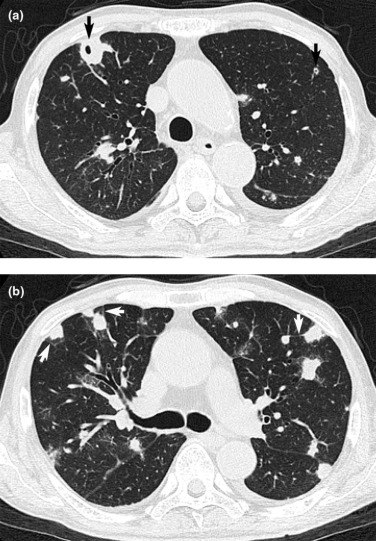
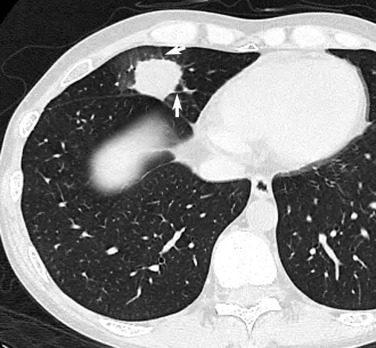
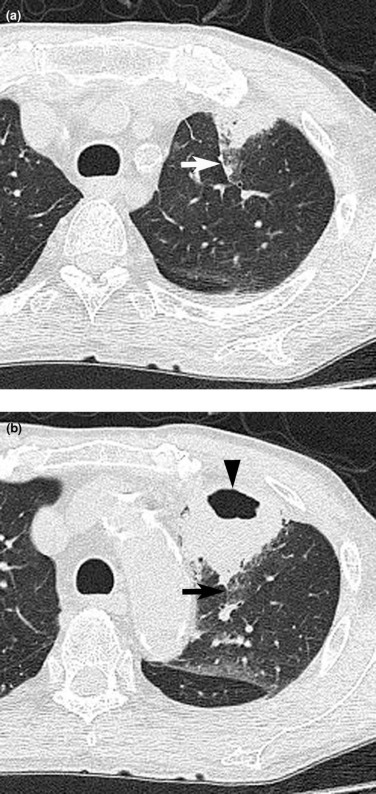
Underlying conditions included respiratory disease ( n = 6, 33.3%), collagen diseases ( n = 5, 27.8%), and diabetes mellitus ( n = 4, 22.2%). All patients showed abnormal HRCT findings, including the presence of a nodule/mass ( n = 17, 94.4%), ground-glass opacity ( n = 14, 77.8%), interlobular septal thickening ( n = 14, 77.8%), and cavitation ( n = 12, 66.7%). Pleural effusion was seen in two patients. There were no cases of lymph node enlargement.
Conclusions
Among the HRCT findings in patients with pneumonia, a nodule/mass with interlobular septal thickening and/or cavitation are suggestive of pulmonary nocardiosis.
Introduction
Nocardia are a group of aerobic, Gram-positive, partially acid-fast species that are ubiquitous in the environment as saprophytic components in dust, soil, water, decaying vegetation, and stagnant matter. They are not part of the normal human flora nor are they a common laboratory contaminant . Human infection mainly occurs through direct inoculation of the skin or by inhalation.
People susceptible to Nocardia infections include recipients of lung, heart, bone marrow, and kidney transplants; human immunodeficiency virus (HIV)-infected individuals; chronic steroid users; and patients with malignancies . However, as many as one-third of patients with nocardiosis have normal immunity . Clinically, pulmonary nocardiosis presents as pneumonia with nonspecific symptoms such as productive cough, fever, dyspnea, chills, weight loss, fatigue, and hemoptysis, with symptoms developing over a period of weeks to months . There are no suggestive clinical manifestations, and nocardiosis is difficult to diagnose .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics and Underlying Conditions
M, F 11, 7 Age (year) Range 39–83 Mean 67.9 Community acquired 15 (83.3) Nosocomial 3 (16.7) Underlying conditions Respiratory disease 6 (33.3) Collagen disease 5 (27.8) Diabetes mellitus 4 (22.2) Smoking habit 4 (22.2) Hypertension 3 (16.7) Alcoholic 2 (11.1) Nephrotic syndrome 1 (5.6) Malignancy 1 (5.6) Presenting symptoms Fever 7 (38.9) Cough 7 (38.9) Sputum 4 (22.2) Dyspnea 4 (22.2) Chest pain 1 (5.6)
Note: Data in parentheses are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Examination
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Image Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Clinical Features
Get Radiology Tree app to read full this article<
CT Patterns
Get Radiology Tree app to read full this article<
Table 2
Thoracic CT Findings in 18 Patients
Findings No. of Patients Nodule/Mass 17 (94.4) Ground-glass opacity 14 (77.8) Interlobular septal thickening 14 (77.8) Cavitation 12 (66.7) Consolidation 6 (33.3) Bronchial wall thickening 1 (5.6) Intralobular reticular opacity 0 (0) Mucoid impaction 0 (0) Centrilobular nodules 0 (0) Pleural effusion 2 (11.1) Lymph node enlargement 0 (0)
CT, computed tomography.
Note: Data in parentheses are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Disease Distribution
Get Radiology Tree app to read full this article<
Pleural Effusion and Lymph Nodes
Get Radiology Tree app to read full this article<
Follow-up
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. McNeil M.M., Brown J.M.: The medically important aerobic actinomycetes: epidemiology and microbiology. Clin Microbiol Rev 1994; 7: pp. 357-417.
2. Hui C.H., Au V.W.K., Rowland K., et. al.: Pulmonary nocardiosis re-visited: experience of 35 patients at diagnosis. Respir Med 2003; 97: pp. 709-717.
3. Filice G.A.: Nocardiosis in persons with human immunodeficiency virus infection, transplant recipients, and large geographically defined populations. J Lab Clin Med 2005; 145: pp. 156-162.
4. Raby N., Forbes G., Williams R.: Nocardia infection in patients with liver transplants or chronic liver disease: radiologic findings. Radiology 1990; 174: pp. 713-716.
5. Beaman B.L., Burnside J., Edwards B., et. al.: Nocardia infection in the United States, 1972-1974. J Infect Dis 1976; 134: pp. 286-289.
6. Lederman E.R., Crum N.F.: A case series and focused review of nocardiosis: clinical and microbiologic aspects. Medicine 2004; 83: pp. 300-313.
7. Uttamchandani R.B., Daikos G.L., Reyes R.R., et. al.: Nocardiosis in 30 patients with advanced human immunodeficiency virus infection: clinical features and outcome. Clin Infect Dis 1994; 18: pp. 348-353.
8. Menendez R., Cordero P.J., Santos M., et. al.: Pulmonary infection with Nocardia species: a report of 10 cases and review. Eur Respir J 1997; 10: pp. 1542-1546.
9. Batista M.V., Pierrotti L.C., Abdala E., et. al.: Endemic and opportunistic infections in Brazilian solid organ transplant recipients. Trop Med Int Health 2011; 16: pp. 1134-1142.
10. Chen J., Zhou H., Xu P., et. al.: Clinical and radiographic characteristics of pulmonary nocardiosis: clues to earlier diagnosis. PLoS ONE 2014; 9: e90724
11. Wang H.K., Sheng W.H., Hung C.C., et. al.: Clinical characteristics, microbiology, and outcomes for patients with lung and disseminated nocardiosis in a tertiary hospital. J Formos Med Assoc 2013; S0929-6646: pp. 264-267.
12. Blackmon K.N., Ravenel J.G., Gomez J.M., et. al.: Pulmonary nocardiosis computed tomography features at diagnosis. J Thorac Imaging 2011; 26: pp. 224-229.
13. Buckley J.A., Padhani A.R., Kuhlman J.E.: CT findings of pulmonary nocardiosis. J Comput Assist Tomogr 1995; 19: pp. 726-732.
14. Yoon H.K., Im J.G., Ahn J.M., et. al.: Pulmonary nocardiosis: CT findings. J Comput Assist Tomogr 1995; 19: pp. 52-55.
15. Oszoyoglu A.A., Kirsch J., Mohammed T.L.: Pulmonary nocardiosis after lung transformation—CT findings in 7 patients and review of the literature. J Thorac Imaging 2007; 22: pp. 143-148.
16. Tsujimoto N., Saraya T., Kikuchi K., et. al.: High-resolution CT findings of patients with pulmonary nocardiosis. J Thorac Dis 2012; 4: pp. 577-582.
17. Kanne J.P., Yandow D.R., Mohammed T.L., et. al.: CT findings of pulmonary nocardiosis. AJR Am J Roentgenol 2011; 197: pp. 266-272.
18. Torres A., Serra-Batlles J., Ferrer A., et. al.: Severe community-acquired pneumonia: epidemiology and prognostic factors. Am Rev Respir Dis 1991; 144: pp. 312-318.
19. Jong G.M., Hsiue T.R., Chen C.R., et. al.: Rapidly fatal outcome of bacteremic Klebsiella pneumoniae pneumonia in alcoholics. Chest 1995; 107: pp. 214-217.
20. Hansell D.M., Bankier A.A., MacMahon H., et. al.: Fleischner Society: glossary of terms for thoracic imaging. Radiology 2008; 246: pp. 697-722.
21. Cooper C.J., Said S., Popp M., et. al.: A complicated case of an immunocompetent patient with disseminated nocardiosis. Infect Dis Rep 2014; 6: pp. 5327.
22. Martinez Tomas R., Menensez Villanueva R., Reyes Caldaza S., et. al.: Pulmonary nocardiosis: risk factors and outcomes. Respirology 2007; 12: pp. 394-400.
23. Georghiou P.R., Blacklock Z.M.: Infection with Nocardia species in Queensland: a review of 102 isolates. Med J Aust 1992; 156: pp. 692-697.
24. Ambrosioni J., Lew D., Garbino J.: Nocardiosis: update clinical review and experience at a tertiary center. Infection 2010; 38: pp. 89-97.
25. Feigin D.S.: Nocardiosis of the lung: chest radiographic findings in 21 cases. Radiology 1986; 159: pp. 9-14.
26. Dodd J.D., de Jong P.A., Levy R.D., et. al.: Conventional high-resolution CT versus contiguous multidetector CT in the detection of bronchiolitis obliterans syndrome in lung transplant recipients. J Thorac Imaging 2008; 23: pp. 235-243.
27. Okada F., Ando Y., Wakisaka M., et. al.: Chlamydia pneumoniae and Mycoplasma pneumoniae pneumonia: comparison of clinical findings and CT findings. J Comput Assist Tomogr 2005; 29: pp. 626-632.
28. Okada F., Ando Y., Tanoue S., et. al.: Radiological findings in acute Haemophilus influenzae pulmonary infection. Br J Radiol 2012; 85: pp. 121-126.
29. Okada F., Ando Y., Nakayama T., et. al.: Pulmonary thin-section CT findings in acute Moraxella catarrhalis pulmonary infection. Br J Radiol 2011; 84: pp. 1109-1114.
30. Morikawa K., Okada F., Ando Y., et. al.: Methicillin-resistant Staphylococcus aureus and methicillin-susceptible S. aureus pneumonia: comparison of clinical and thin-section CT findings. Br J Radiol 2012; 85: pp. e168-e175.
31. Okada F., Ando Y., Matsushita S., et. al.: Thin-section computed tomography findings of patients with acute Streptococcus pneumoniae pneumonia with and without concurrent infection. Br J Radiol 2012; 85: pp. e357-e364.
32. Okada F., Ando Y., Honda K., et. al.: Acute Klebsiella pneumoniae pneumonia alone and with concurrent infection: comparison of clinical and thin-section CT findings. Br J Radiol 2010; 83: pp. 854-860.
33. Okada F., Ono A., Ando Y., et. al.: High-resolution CT findings in Streptococcus milleri pulmonary infection. Clin Radiol 2013; 68: pp. e331-e337.
34. Okada F., Ono A., Ando Y., et. al.: Thin-section CT findings in Pseudomonas aeruginosa pulmonary infection. Br J Radiol 2012; 85: pp. 1533-1538.
35. van Kralingen K.W., Hekker T.A., Bril H., et. al.: Haemoptysis and an abnormal X-ray after prolonged treatment in the ICU. Eur Respir J 1994; 7: pp. 419-420.
36. Tanaka N., Matsumoto T., Kuramitsu T., et. al.: High resolution CT findings in community-acquired pneumonia. J Comput Assist Tomogr 1996; 20: pp. 600-608.
37. Rubin E., Shin M.S.: Pleural and extrapleural disease in Nocardia infections. J Can Assoc Radiol 1984; 35: pp. 189-191.
38. Presant C.A., Wiernik P.H., Serpick A.A.: Factors affecting survival in nocardiosis. Am Rev Respir Dis 1973; 108: pp. 1444-1448.
39. Beaman B.L., Beaman L.: Nocardia species: host-parasite relationships. Clin Microbiol Rev 1994; 7: pp. 213-264.