
Rationale and Objectives
We sought to evaluate the diagnostic performance of high-resolution magnetic resonance imaging (MRI) and conventional MRI of the knee on a standard–field-strength MRI system compared to arthroscopic findings in patients with suspected meniscal tears.
Materials and Methods
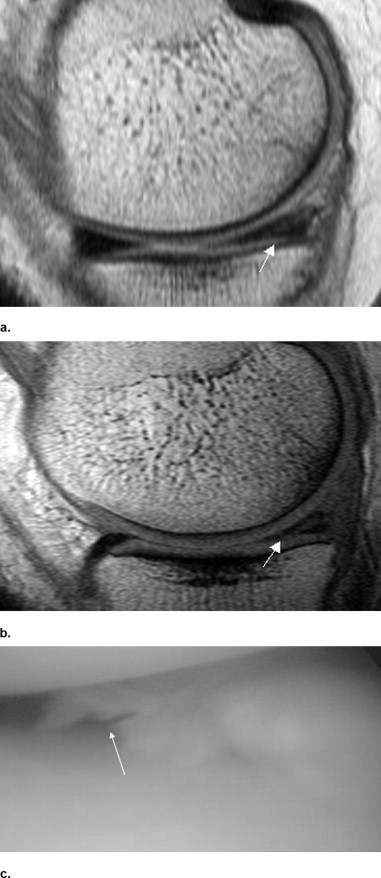
Forty-two patients (20 women, 22 men), referred from the department of trauma surgery, with suspected medial meniscal tears and planned arthroscopy of the knee joint were included in the study. MRI was performed on a 1.0-T MRI scanner with two different protocols: (1) conventional MRI using a circular, polarized knee coil (coil diameter: 17 cm) with a sagittal dual fast spin-echo sequence (repetition time [TR]: 2500 ms; echo time [TE]: first, shortest, second, 120 ms; turbo spin echo [TSE] factor: 12; field of view: 180 mm; matrix: 256 × 512; scan percentage: 100; slice thickness: 3 mm) or (2) high-resolution MRI with a surface dual-loop coil of the medial knee compartment (temporomandibular joint, coil diameter: 8 cm) with a sagittal dual fast spin-echo sequence (TR: 2400 ms; TE: first, shortest; second, 120 ms; TSE factor: 12; field of view: 120 mm; matrix: 512 × 512; slice thickness: 2 mm). The menisci were evaluated on the basis of an adapted score (0 = normal meniscus, 1 = intrameniscal, T2-weighted hyperintense signal, 2 = discontinuity of the surface, 3 = fragmentation). Lesions that received a score of 2 or 3 were graded as meniscal tears. The MRI results were compared to the arthroscopic reports, which represented the gold standard, and the sensitivity of both protocols in detecting a meniscal tear was determined.
Results
Of the 42 patients included in the study, 25 (11 women and 14 men) underwent arthroscopy and all demonstrated a meniscal tear. A meniscal tear was correctly diagnosed in 76% of cases with conventional MRI and in 88% of cases with high-resolution MRI ( P = .0087).
Conclusion
High-resolution MRI, using a surface dual-loop coil and specific sequences, which can be performed on every standard–field-strength MRI scanner, is able to significantly improve diagnostic performance for the detection of a meniscal tear of the knee joint.
Magnetic resonance imaging (MRI) is the most commonly used imaging modality for the diagnosis of a suspected meniscal tear. This imaging technique has proved useful for the visualization of meniscal tears for more than 15 years, with variable accuracy reported in most studies ( ). From a therapeutic viewpoint, an accurate description of a meniscal tear has become increasingly important, with the emphasis on meniscal preservation, repair, and even transplantation, whereas the absence of a normal meniscus can lead to accelerated and irreversible degenerative changes ( ). The diagnosis of a meniscal tear requires high spatial resolution and an optimized signal-to-noise ratio, a slice thickness of, at most, 3 mm, a field of view (FOV) of 16 cm or less, and a matrix size of at least 256 × 192 ( ). Many MR sequences have been used to evaluate meniscal tears, including spin-echo (SE) or fast spin-echo (FSE), proton density (PD) with or without fat saturation, T1, and gradient echo (GRE) ( ). Recent developments with 3-T MRI have not yet been fully evaluated but offer promise for highly accurate meniscal visualization ( ). Despite the growing number of 3-T scanners, there are still many 1- and 1.5-T machines in use, especially in smaller hospitals and private institutions.
Thus, the aim of this study was to evaluate the diagnostic performance of high-resolution MRI with a surface coil and conventional MRI, both performed on a 1-T unit, compared with arthroscopic findings in patients with suspected meniscal tears.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patients and Pathologies
Patient No. Age Sex CMRI HRMRI Localization Surgery 1 38 F 3 3 Post. horn Positive 2 38 M 2 2 Post. horn Positive 3 55 F 2 2 Post. horn Positive 4 35 M 3 3 Ant. horn Positive 5 37 M 2 2 Post. horn Positive 6 29 F 2 2 Post. horn Positive 7 22 M 1 2 Post. horn Positive 8 51 M 2 2 Post. horn Positive 9 28 M 3 3 Post. horn Positive 10 31 M 2 3 Post. horn Positive 11 36 F 2 2 Post. horn Positive 12 51 F 2 2 Post. horn Positive 13 18 F 1 2 Post. horn Positive 14 50 M 3 3 Post. horn Positive 15 31 F 1 1 Post. horn Positive 16 32 F 3 3 Post. horn Positive 17 41 M 3 3 Post. horn Positive 18 50 M 3 3 Post. horn Positive 19 52 F 1 1 Post. horn Positive 20 18 F 3 3 Ant. horn Positive 21 51 M 2 2 Post. horn Positive 22 33 M 1 1 Post. horn Positive 23 31 F 1 2 Post. horn Positive 24 50 M 3 3 Post. horn Positive 25 49 M 2 3 Post. horn Positive
Ant., anterior; CMRI, conventional magnetic resonance imaging; HRMRI, high-resolution magnetic resonance imaging; Post., posterior.

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Fox M.G.: MR imaging of the meniscus: Review, current trends, and clinical implications. Magn Reson Imaging Clin N Am 2007; 15: pp. 103-123.
2. Helms C.A.: The meniscus: Recent advances in MR imaging of the knee. AJR Am J Roentgenol 2002; 179: pp. 1115-1122.
3. Rath E., Richmond J.C.: The menisci: Basic science and advances in treatment. Br J Sports Med 2000; 34: pp. 252-257.
4. Escobedo E.M., Hunter J.C., Zink-Brody G.C., Wilson A.J., Harrison S.D., Fisher D.J.: Usefulness of turbo spin-echo MR imaging in the evaluation of meniscal tears: Comparison with a conventional spin-echo sequence. AJR Am J Roentgenol 1996; 167: pp. 1223-1227.
5. Rubin D.A., Paletta G.A.: Current concepts and controversies in meniscal imaging. Magn Reson Imaging Clin N Am 2000; 8: pp. 243-270.
6. Mink J.H., Levy T., Crues J.V.: Tears of the anterior cruciate ligament and menisci of the knee: MR imaging evaluation. Radiology 1988; 167: pp. 769-774.
7. Magee T., Williams D.: 3.0-T MRI of meniscal tears. AJR Am J Roentgenol 2006; 187: pp. 371-375.
8. Magee T.: Three-tesla MR imaging of the knee. Magn Reson Imaging Clin N Am 2007; 15: pp. 125-132.
9. Von Engelhardt L.V., Schmitz A., Pennekamp P.H., Schild H.H., Wirtz D.C., von Falkenhausen F.: Diagnostics of degenerative meniscal tears at 3-Tesla MRI compared to arthroscopy as reference standard. Arch Orthop Trauma Surg 2008; 128: pp. 451-456.
10. Lotysch M., Mink J., Crues J.V., Schwartz S.A.: Magnetic resonance imaging in the detection of meniscal injuries. Magn Reson Imaging 1986; 4: pp. 94.
11. De Smet A.A., Norris M.A., Yandow D.R., Quintana F.A., Graf B.K., Keene J.S.: MR diagnosis of meniscal tears of the knee: Importance of high signal in the meniscus that extends to the surface. AJR Am J Roentgenol 1993; 161: pp. 101-107.
12. Jee W.H., McCauley T.R., Kim J.M., et. al.: Meniscal tear configurations: Categorization with MR imaging. AJR Am J Roentgenol 2003; 180: pp. 93-97.
13. Rand T., Imhof H., Turetschek K., et. al.: Comparison of low field (0.2T) and high field (1.5T) MR imaging in the differentiation of torned from intact menisci. Eur J Radiol 1999; 30: pp. 22-27.
14. Parizel P.M., Dijkstra H.A., Geenen G.P., et. al.: Low-field versus high-field MR imaging of the knee: A comparison of signal behaviour and diagnostic performance. Eur J Radiol 1995; 19: pp. 132-138.
15. Cotten A., Delfaut E., Demondion X., et. al.: MR imaging of the knee at 0.2 and 1.5 T: Correlation with surgery. AJR Am J Roentgenol 2000; 174: pp. 1093-1097.
16. Marlovits S., Striessnig G., Resinger C.T., et. al.: Definition of pertinent parameters for the evaluation of articular cartilage repair tissue with high-resolution magnetic resonance imaging. Eur J Radiol 2004; 52: pp. 310-319.
17. Van Den Steen M., De Maeseneer M., Hoste M., Vanderdood K., De Ridder F., Osteaux M.: Comparison of surface coil and knee coil for evaluation of the patellar cartilage by MR imaging. Eur J Radiol 2003; 47: pp. 43-46.
18. Trattnig S., Millington S.A., Szomolanyi P., Marlovits S.: MR imaging of osteochondral grafts and autologous chondrocyte implantation. Eur Radiol 2007; 17: pp. 103-118.
19. Rubin D.A., Kneeland J.B., Listerud J., Underberg-Davis S.J., Dalinka M.K.: MR diagnosis of meniscal tears of the knee: Value of fast spin-echo vs conventional spin-echo pulse sequences. AJR Am J Roentgenol 1994; 162: pp. 1131-1135.
20. De Smet A.A., Tuite M.J.: Use of the “two-slice-touch” rule for the MRI diagnosis of meniscal tears. AJR Am J Roentgenol 2006; 187: pp. 911-914.
21. Cheung L.P., Li K.C., Hollett M.D., Bergman A.G., Herfkens R.J.: Meniscal tears of the knee: Accuracy of detection with fast spin-echo MR imaging and arthroscopic correlation in 293 patients. Radiology 1997; 203: pp. 508-512.
22. Schäfer F.K., Schäfer P.J., Brossmann J., et. al.: Value of fat-suppressed proton-density-weighted turbo spin-echo sequences in detecting meniscal lesions: Comparison with arthroscopy. Acta Radiol 2006; 47: pp. 385-390.
23. Kowalchuk R.M., Kneeland J.B., Dalinka M.K., Siegelman E.S., Dockery W.D.: MRI of the knee: Value of short echo time fast spin-echo using high performance gradients versus conventional spin-echo imaging for the detection of meniscal tears. Skeletal Radiol 2000; 29: pp. 520-524.
24. Magee T., Williams D.: Detection of meniscal tears and marrow lesions using coronal MRI. AJR Am J Roentgenol 2004; 183: pp. 1469-1473.
25. Tarhan N.C., Chung C.B., Mohana-Borges A.V., Hughes T., Resnick D.: Meniscal tears: Role of axial MRI alone and in combination with other imaging planes. AJR Am J Roentgenol 2004; 183: pp. 9-15.