
We describe our method of exposing radiology residents to root cause analysis. Our interactive case-based, small-group teaching session uses a flipped classroom approach which allows the session to focus primarily on working through the case in small groups. This methodology can be easily integrated at other institutions.
Background
Error has been long recognized as ubiquitous to the practice of medicine. In the Institute of Medicine’s report To Err is Human: Building a Safer Healthcare System, nearly 100,000 deaths annually can be attributed to medical error . Learning from our mistakes is one aspect of error reduction. Root cause analysis (RCA) is an established method by which to systematically analyze the contributing factors accounting for a medical error and to guide implementation of system-wide change to prevent future mistakes. The Joint Commission for Accreditation of Healthcare Organizations (JCAHO) requires that an RCA be completed within 45 days of any major or sentinel event . A sentinel event is defined by JCAHO as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof . For radiology, examples of sentinel events would include wrong site procedures, retained foreign bodies, or prolonged fluoroscopy resulting in >1500 rads cumulative dose to a single field.
At its core, RCA is a retrospective process used to identify errors underlying variation in performance and allows for the development of effective strategies to decrease the likelihood of similar adverse events occurring in the future . The two major categories of error include active and latent error. Active errors occur during the interaction of people and complex systems. Latent errors represent inherent system failures. As active errors are difficult to predict, RCA aims to identify and reduce systemic errors that can be rectified preventing adverse events. RCA entails five key steps: (1) define the problem and gather data; (2) identify, classify, and prioritize possible contributors; (3) identify root causes; (4) generate solutions; and (5) implement system change and disseminate results.
In our department, introducing residents to RCA is part of a broader training in quality, safety, and other practice management skills. Resident exposure to these areas includes a dedicated lecture series, mandatory mentored Practice Quality Improvement (PQI) projects, and the opportunity to join our department’s Radiology Leadership Academy. Exposure to RCA was deemed important as not only will residents be future leaders in our field, but also the ability to conduct an RCA can fulfill a component of the American Board of Radiology’s Maintenance of Certifications process and plays a role in Systems-Based Practice, an Accreditation Council for Graduate Medical Education core competency . To engage residents, we designed an interactive case-based, small-group teaching session that occurs during dedicated didactic time. In this article, we highlight how we conduct this interactive session using a sentinel event and applying principles of RCA.
Choosing the Case
Selection of an appropriate case is the important first step in creating a case-based, small-group teaching session. The case must be comprehensive to cover all stages in the process. The case presented later, a case of wrong site injection, was selected by a consensus of the authors through a review of our department’s quality improvement database . This database consists of all imaging cases entered in real-time by any departmental trainee or faculty member. Cases are de-identified and some details are changed to protect identities and maximize the learning process. Although we certainly welcome resident input to case selection, the reality is that most residents do not personally experience an RCA during their training, and therefore, we believe that this simulated exercise provides an opportunity to develop this critical skill set.
Case Summary—Wrong Site Injection
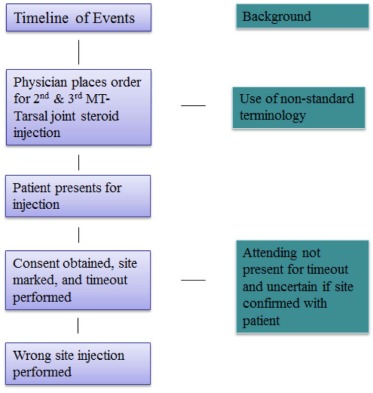
A 53-year-old male with chronic foot pain presented for a fluoroscopically guided steroid injection of his right foot after having experienced no pain relief following an injection performed in the orthopedic office. After obtaining written informed consent and performing a time-out, the radiology fellow and attending radiologist successfully injected 40 mg of Depomedrol and 0.5% Sensorcaine into the second and third metatarsophalangeal joints (MTP). After the procedure was completed, the patient commented that the band-aid was in a different location compared to the prior procedure. A review of the requisition showed the order to be “please inject steroids into the 2nd and 3rd MTT joints.” After realizing that the wrong joints were injected, an apology was issued and the correct joints were injected.
Analyzing the Case
Get Radiology Tree app to read full this article<
Table 1
The Five Major Tasks of Root Cause Analysis
Task 1: Define the problem and gather data and evidence.
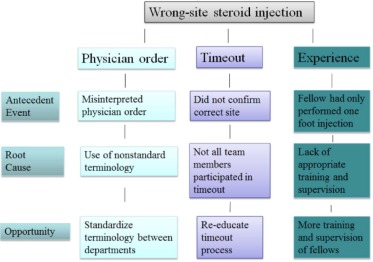
Task 2: Identify, classify, and prioritize possible contributors.
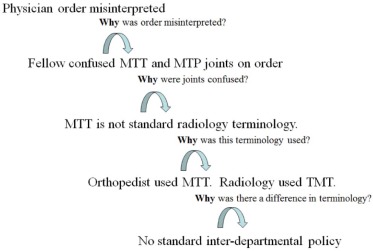
Task 3: Identify root causes.
Task 4: Generate solutions.
Task 5: Implement solutions and disseminate results.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Group 1: Define the Problem and Gather Data and Evidence
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Group 2: Identify, Classify, and Prioritize Possible Contributors
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Group 3: Identify Root Causes
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Group 4: Generate Solutions
Get Radiology Tree app to read full this article<
Group 5: Implement Solutions and Disseminate Results
Get Radiology Tree app to read full this article<
Presenting the Findings
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Institute of Medicine : Institute of Medicine (IOM) Report. To err is human. Available at: https://www.iom.edu/~/media/Files/Report%20Files/1999/To-Err-is-Human/To%20Err%20is%20Human%201999%20%20report%20brief.pdf Accessed November 11, 2015
2. The Joint Commission : Sentinel events (SE). Available at: http://www.jointcommission.org/assets/1/6/CAMH_2012_Update2_24_SE.pdf Accessed January 9, 2016
3. American Board of Radiology Maintenance of Certification : Available at: http://www.theabr.org/moc-dr-comp4 Accessed February 9, 2016
4. Accreditation Council for Graduate Medical Education : The diagnostic radiology milestone project. Available at: https://www.acgme.org/acgmeweb/Portals/0/PDFs/Milestones/DiagnosticRadiologyMilestones.pdf Accessed February 9, 2016
5. Kruskal J.B., Yam C.S., Sosna J., et. al.: Implementation of online radiology quality assurance reporting system for performance improvement: initial evaluation. Radiology 2006; 241: pp. 518-527.
6. Brook O.R., Kruskal J.B., Eisenber R., et. al.: Root cause analysis: learning from adverse safety events. Radiographics 2015; 35: pp. 1655-1667.
7. Choksi V.R., Marn C., Piotrowski M.M., et. al.: Illustrating the root-cause-analysis process: creation of a safety net with a semiautomated process for the notification of critcial findings in diagnostic imaging. J Am Coll Radiol 2005; 2: pp. 768-776.
8. Federal Aviation Administration : FAA system safety handbook. Available at: https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/risk_management/ss_handbook/media/Chap9_1200.pdf Accessed February 8, 2016
9. Kruskal J.B., Eisenberg R.E., Sosna J., et. al.: Quality improvement in radiology: basic principles and tools required to achieve success. Radiographics 2011; 31: pp. 1499-1509.
10. Kruskal J.B., Siewert B., Anderson S., et. al.: Quality initiatives managing an acute adverse event in a radiology department. Radiographics 2008; 28: pp. 1237-1250.