
Rationale and Objectives
To assess the effect of short-term corticosteroid premedication on serum glucose in hospitalized patients.
Materials and Methods
Serum glucose in adult inpatients receiving corticosteroid premedication before a radiology study was compared to serum glucose in nonpremedicated controls between May 1, 2008, and September 12, 2009. Patients were categorized by type of nonionic contrast medium (intravenous [IV] or none) and route of corticosteroid premedication (oral, IV, none). Diabetes mellitus (types I and II) was evaluated as an independent risk factor. Patients without glucose estimations before and after premedication were excluded. Results were analyzed with analysis of variance and a stepwise linear regression analysis.
Results
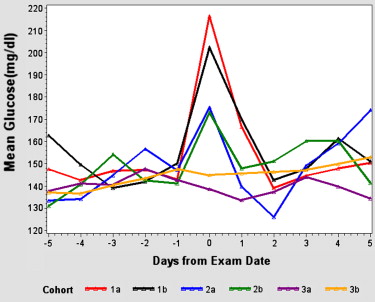
There were 390 corticosteroid premedication episodes in 390 patients; 873 examinations in 844 patients served as controls. Cohorts receiving corticosteroid premedication experienced a brief (24–48 hour) increase in mean maximum postbaseline serum glucose (IV, +81 mg/dL; oral, +70 mg/dL) that was greater than the increase in nonpremedicated controls (+46 mg/dL). Type I (+144 mg/dL) and type II (+108 mg/dL) diabetics had a greater elevation than nondiabetics (+34 mg/dL). Both corticosteroid premedication (IV, P = .02; oral, P = .01) and diabetes mellitus (type I, P = .0002; type II, P < .0001) were significant independent risk factors of hyperglycemia. The use of nonionic intravascular contrast medium was not ( P = .7). There was no significant difference between IV and oral premedication ( P = .6), or type I and type II diabetes mellitus ( P = .8).
Conclusions
Diabetes mellitus (type I and type II) and corticosteroid premedication (oral and IV) are significant independent risk factors for the development of brief hyperglycemia near the time of inpatient radiology studies.
The American College of Radiology recommends that corticosteroid premedication be administered before intravascular contrast medium injection in patients at increased risk for an allergic-like reaction . This is done to reduce the likelihood of a severe allergic-like reaction, although no trials have demonstrated a conclusive risk reduction for severe reactions . The risks of corticosteroids are presumed to be lower than the risks of a potential reaction, but this favorable risk–benefit relationship has been assumed rather than rigorously validated. For example, corticosteroids are known to cause hyperglycemia , and hyperglycemia secondary to a variety of causes has been shown to confer an increased morbidity and mortality in critically ill patients . Diabetic patients are at greatest risk for the development of hyperglycemia from their impaired ability to use glucose. There is a paucity of published data analyzing the risks of corticosteroid premedication for imaging studies, particularly in the at-risk diabetic population. The purpose of our study was to assess the effect of short-term corticosteroid premedication on serum glucose levels in hospitalized patients.
Subjects and methods
Before the initiation of this investigation, institutional review board approval was obtained. The study was carried out in compliance with the US Health Insurance Portability and Accountability Act. Patient informed consent was not required based on institutional policy and the retrospective nature of this investigation.
Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Characteristics of the Six Study Cohorts
Cohort Steroids Contrast Number of Index Studies Patients ( n ) Mean Age (y) Minimum Age Maximum Age Type I DM Type II DM 1a Oral IV 193 193 58 18 96 2 57 1b Oral None 132 132 58 27 95 2 38 2a IV IV 42 42 61 26 91 2 11 2b IV None 23 23 60 25 82 0 7 3a None IV 428 412 53 18 91 5 77 3b None None 445 432 58 18 95 6 91
DM, diabetes mellitus; IV, intravenous; steroids, the type of corticosteroid premedication; contrast, iodinated nonionic contrast administration during computed tomography or angiography.
Get Radiology Tree app to read full this article<
Index Studies
Get Radiology Tree app to read full this article<
Corticosteroid Premedication
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Exams that were Preceded by Corticosteroid Premedication in the Absence of Intravascular Iodinated Nonionic Contrast Medium Administration: Cohorts 1b and 2b
Study type Cohort 1b: Oral Corticosteroids No Contrast Material Cohort 2b: IV Corticosteroids No Contrast Material Number of Index Studies Patients ( n ) Number of Index Studies Patients ( n ) Noncontrast CT 3 3 4 4 Fluoroscopy 2 2 2 2 Interventional 8 8 1 1 Gadolinium-enhanced MR 106 106 14 14 Noncontrast MR 4 4 0 0 Study canceled 8 8 2 2 Myelography 1 1 0 0
Fluoroscopy, fluoroscopic examination during the intra-cavitary administration of contrast medium; interventional, interventional procedures that did not involve intravascular iodinated contrast medium (eg, CO 2 angiography, CT, or ultrasound-guided biopsy); MR, magnetic resonance; noncontrast CT, computed tomography without intravascular iodinated contrast administration.
Get Radiology Tree app to read full this article<
Periprocedural and Baseline Serum Glucose
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Intravascular Iodinated Contrast Media
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Population
Get Radiology Tree app to read full this article<
Baseline Serum Glucose
Get Radiology Tree app to read full this article<
Table 3
Baseline and Maximum Postbaseline Serum Glucose by cohort and Demographic Subset
Baseline Maximum Postbaseline Cohort Steroids Contrast_n_ Mean Minimum Maximum Mean Minimum Maximum 1a Oral IV 193 147 72 457 214 65 601 DMI 2 220 197 243 473 344 601 DMII 57 193 80 457 305 100 601 No DM 134 126 72 344 170 65 469 1b Oral None 132 138 78 352 212 83 601 DMI 2 222 189 254 278 193 362 DMII 38 176 85 352 300 98 601 No DM 92 121 78 183 172 83 601 2a IV IV 42 139 79 308 221 107 601 DMI 2 234 159 308 347 287 406 DMII 11 155 120 205 298 153 601 No DM 29 125 79 203 182 107 334 2b IV None 23 142 97 282 220 105 435 DMI 0 NA NA NA NA NA NA DMII 7 173 124 282 283 136 435 No DM 16 129 97 183 192 105 425 3a None IV 428 125 61 463 168 63 1321 DMI 5 266 129 463 314 168 537 DMII 77 165 75 372 263 110 1321 No DM 346 115 61 272 142 63 601 3b None None 445 129 59 351 178 77 864 DMI 6 131 97 180 359 219 576 DMII 91 161 82 351 263 99 601 No DM 348 121 59 271 150 77 864
All serum glucose values are measured in mg/dL.
Contrast, route of administration of nonionic intravascular contrast material; DMI, type I diabetes; DMII, type II diabetes; no DM, not having diabetes; IV, intravenous; none, no nonionic intravascular contrast medium administered; NA, not applicable; steroids, corticosteroid premedication.
Get Radiology Tree app to read full this article<
Maximum Postbaseline Serum Glucose
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Regression Analyses
Get Radiology Tree app to read full this article<
Table 4
Univariate and Multivariate Logistic Regression Analyses of Multiple Variables and their Effect on Postbaseline Serum Glucose
Univariate Analyses Variable Effect_P_ Value Age Increase .02 † Any premedication (IV or oral) Increase <.0001 † IV vs. no premedication ∗ Increase .007 † IV vs. oral premedication ∗ None .6 No vs. oral premedication ∗ Decrease .0002 † Any diabetes (type I or type II) Increase <.0001 † Type I vs. type II diabetes ∗ None .8 Type I diabetes vs. nondiabetic ∗ Increase .0001 † Type II diabetes vs. nondiabetic ∗ Increase <.0001 † Intravascular iodinated contrast IV vs. no iodinated contrast ∗ None .8
Multivariate Analysis Variable Effect_P_ Value IV vs. no premedication ∗ Increase .02 † IV vs. oral premedication ∗ None .5 No vs. oral premedication ∗ Decrease .01 † Type I vs. type II diabetes ∗ None .8 Type I diabetes vs. nondiabetic ∗ Increase .0002 † Type II diabetes vs. nondiabetic ∗ Increase <.0001 †
Effect, directionality of effect on postbaseline serum glucose; IV, intravenous.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. American College of Radiology: ACR practice guideline for the use of intravascular contrast media.Practice guidelines and technical standards, 2007.2007.American College of RadiologyReston, Va:pp. 73-78.
2. Morcos S.K.: Acute serious and fatal reactions to contrast media: our current understanding. Br J Radiol 2005; 78: pp. 686-693.
3. Greenberger P.A., Halwig J.M., Patterson R., et. al.: Emergency administration of radiocontrast media in high-risk patients. J Allergy Clin Immunol 1986; 77: pp. 630-634.
4. Greenberger P.A., Patterson R.: The prevention of immediate generalized reactions to radiocontrast media in high-risk patients. J Allergy Clin Immunol 1991; 97: pp. 867-872.
5. Greenberger P.A., Patterson R., Simon R., et. al.: Pretreatment of high-risk patients requiring radiographic contrast media studies. J Allergy Clin Immunol 1981; 67: pp. 185-187.
6. Lasser E.C., Berry C.C., Mishkin M.M., et. al.: Pretreatment with corticosteroids to prevent adverse reactions to nonionic contrast media. AJR Am J Roentgenol 1994; 162: pp. 523-526.
7. Lasser E.C., Berry C.C., Talner L.B., et. al.: Pretreatment with corticosteroids to alleviate reactions to intravenous contrast material. N Engl J Med 1987; 317: pp. 845-849.
8. Lieberman P., Kemp S.F., Oppenheimer J., et. al.: The diagnosis and management of anaphylaxis: an updated practice primer. J Allergy Clin Immunol 2005; 115: pp. S483-S523.
9. Buchman A.L.: Side effects of corticosteroid therapy. J Clin Gastroenterol 2001; 33: pp. 289-294.
10. Van den Berghe G., Wilmer A., Hermans G., et. al.: Intensive insulin therapy in the medical ICU. N Engl J Med 2006; 354: pp. 449-461.
11. Van den Berghe G., Wouters P., Weekers F., et. al.: Intensive insulin therapy in critically ill patients. N Engl J Med 2001; 345: pp. 1359-1367.
12. Krinsley J.S.: Association between hyperglycemia and increased hospital mortality in a heterogenous population of critically ill patients. Mayo Clin Proc 2003; 78: pp. 1471-1478.
13. Inzucchi S.E.: Management of hyperglycemia in the hospital setting. N Engl J Med 2006; 355: pp. 1903-1911.
14. Trence D.L., Kelly J.L., Hirsch I.B.: The rationale and management of hyperglycemia for in-patients with cardiovascular disease: time for change. J Clin Endocrinol Metab 2003; 88: pp. 2430-2437.
15. Garber A.J., Moghissi E.S., Bransome E.D., et. al.: American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract 2004; 10: pp. 77-82.
16. Greenberger P.A., Patterson R., Radin R.C.: Two pre-treatment regimes for high-risk patients receiving radiographic contrast media. J Allergy Clin Immunol 1984; 74: pp. 540-543.
17. Katayama H., Yamaguchi K., Kozuka T., et. al.: Adverse reactions to ionic and nonionic contrast media: a report from the Japanese committee on the safety of contrast media. Radiology 1990; 175: pp. 621-628.
18. Cohan R.H., Ellis J.H., Dunnick N.R.: Use of low-osmolar agents and premedication to reduce the frequency of adverse reactions to radiographic contrast media: a survey of the Society of Uroradiology. Radiology 1995; 194: pp. 357-364.
19. O’Malley R, Cohan RH, Caoili EM, et al. Use of premedication prior to intravenous administration of iodinated and gadolinium based contrast material: a survey of SUR members. Society of Uroradiology Annual Meeting, oral presentation, 2010.
20. Davenport M.S., Cohan R.H., Caoili E.M., et. al.: Repeat contrast medium reactions in premedicated patients: frequency and severity. Radiology 2009; 253: pp. 372-379.
21. Davenport M.S., Cohan R.H., Caoili E.M., et. al.: Hyperglycemic consequences of corticosteroid premedication in an outpatient population. AJR Am J Roentgenol 2010; 194: pp. W483-W488.
22. Boyd R., Leigh B., Stuart P.: Capillary versus venous bedside blood glucose estimations. Emerg Med J 2005; 22: pp. 177-179.
23. Kempke K., Price D., Ellison J., et. al.: Capillary and venous blood glucose concentrations measured during intravenous insulin and glucose infusion: a comparison of steady and dynamic states. Diabetes Technol Ther 2009; 11: pp. 669-674.
24. Colagiuri S., Sandbaek A., Carstensen B.: Comparability of venous and capillary glucose measurements in blood. Diabet Med 2003; 20: pp. 953-956.