
Rationale and Objectives
The aim of this study was to assess the findings of chest radiography and high-resolution computed tomography in patients requiring intensive care unit treatment for severe H1N1 virus pneumonia.
Materials and Methods
In 2009, 10 patients required treatment in an intensive care unit for confirmed H1N1 pneumonia. All patients underwent chest radiography and high-resolution computed tomography. All 10 patients required mechanical ventilation because of respiratory failure. Nine patients presented with severe acute respiratory distress syndrome, and one patient died. Four patients underwent extracorporeal membrane oxygenation (ECMO) therapy. The results of chest radiography and high-resolution computed tomographic scans of these patients were systematically analyzed.
Results
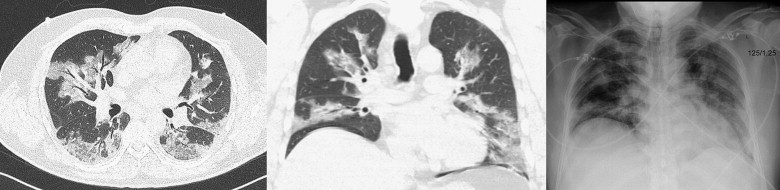
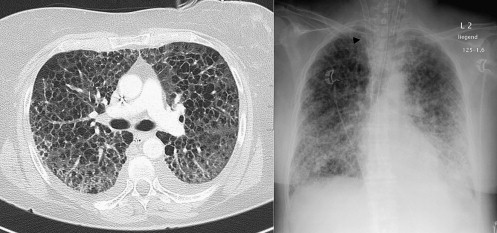
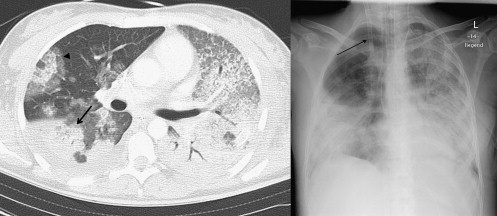
The mean age of all patients was 44.1 ± 12.3 years. All 10 patients showed abnormal results on chest radiography. The radiographic abnormalities were bilateral and multifocal in 10 patients. The predominant radiographic findings were consolidations ( n = 9), ground-glass opacities ( n = 8), and reticular opacities ( n = 2). The most frequent computed tomographic findings at presentation consisted of bilateral ground-glass opacities ( n = 9), pleural effusion ( n = 9), areas of consolidation ( n = 8), interstitial marking ( n = 8), and crazy paving ( n = 4). All patients undergoing ECMO therapy showed extensive bilateral ground-glass opacities, multifocal areas of consolidation, and crazy paving. Pleural effusion was present in three of four patients undergoing ECMO therapy.
Conclusion
Patients requiring treatment in an intensive care unit for severe H1N1 pneumonia are at high risk for developing acute respiratory distress syndrome and frequently require ECMO therapy.
Influenza virus types A and B account for the majority of viral pneumonias in immunocompetent adults . In April 2009, a new strain of human influenza A (H1N1) virus was identified in Mexico and was characterized by a unique combination of gene segments that had not been previously identified among human or swine influenza A viruses . Mexico was the first country to show a sharp increase in reports of patients requiring hospitalization for pneumonia and an unusual series of deaths, leading to the suspicion that a new influenza virus strain was in circulation . As of July 31, 2009, 168 countries and overseas territories or communities had each reported at least one laboratory-confirmed case of pandemic H1N1 influenza, with a total of 162,380 reported cases, including ≥9596 deaths through December 11, 2009 . Consequently, a level 6 pandemic was declared by the World Health Organization.
The clinical symptoms, in the greatest number of patients, consist of mild clinical presentation with influenza-like illness . However, a small percentage of patients with H1N1 virus pneumonia may develop acute respiratory distress syndrome (ARDS) or severe cardiopulmonary failure despite the use of intensive care unit (ICU) treatment. Extracorporeal membrane oxygenation (ECMO) is a well-established option to rescue these severely ill patients.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Population
Get Radiology Tree app to read full this article<
Table 1
Summary of Clinical, Laboratory, Radiographic, and High-resolution Computed Tomographic Findings in 10 Patients with Confirmed H1N1 Virus Pneumonia and Respiratory Failure
Patient Age (y) Sex Preexisting Disease Radiography HRCT ECMO ARDS Leukocytes LDH (U/L) CRP (mg/L) Outcome 1 51 F — Bilateral, multifocal; GGO++; cons+++ Cons patchy+++; GGO++; interstitial markings+ 0 + Normal 1338 395 Died 2 56 F — Bilateral, multifocal; reticular opacities+++; cons++ GGO++; interstitial markings+; crazy paving; cons+; pleural effusion + + Normal 1205 305.9 Discharged 3 51 M — Bilateral, multifocal; cons++ Cons++; GGO+; pleural effusion; atelectasis subtotal left 0 + Leukopenia 233 250.7 Discharged 4 31 M Down syndrome — GGO++; interstitial markings+; atelectasis; pleural effusion 0 + Leukopenia 282 342 Discharged 5 43 M — Bilateral, multifocal; cons++; nodular opacities+ GGO+++; pleural effusion 0 + Leukopenia 662 117.4 Discharged 6 32 F von Willebrand disease bilateral, multifocal; cons+++; GGO+++ GGO+++; cons+++; crazy paving; pleural effusion + + Normal 545 265.5 Discharged 7 27 F Type 1 diabetes Bilateral, multifocal; cons+++; GGO+++ GGO+++; cons+++; crazy paving; pleural effusion + + Leukocytosis 411 371.3 Discharged 8 65 M — Bilateral, multifocal; cons+; GGO+++; reticular opacities+ GGO+++; pleural effusion 0 + Leukocytosis 1785 10.8 Discharged 9 43 M — Bilateral, multifocal; GGO+++; cons+ GGO+++; cons+++; pleural effusion 0 + Leukocytosis 821 290 Discharged 10 54 M — Bilateral, multifocal; cons+++; GGO+++ GGO+++; cons+++; crazy paving; pleural effusion + + Leukocytosis 1640 355 Discharged
ARDS, acute respiratory distress syndrome; cons, consolidation; CRP, C-reactive protein; GGO, ground-glass opacity; ECMO, extracorporeal membrane oxygenation; HRCT, high-resolution computed tomography; LDH, lactate dehydrogenase; +, low predominance; ++, moderate predominance; +++, extensive predominance.
Get Radiology Tree app to read full this article<
Imaging Techniques and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kim E.A., Lee K.S., Primack S.L., et. al.: Viral pneumonias in adults: radiologic and pathologic findings. Radiographics 2002; 22: pp. S137-S149.
2. Zimmer S.M., Burke D.S.: Historical perspective—emergence of influenza A (H1N1) viruses. N Engl J Med 2009; 361: pp. 279-285.
3. Perez-Padilla R., de la Rosa-Zamboni D., Ponce de Leon S., et. al.: Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med 2009; 361: pp. 680-689.
4. Petrosillo N., Di Bella S., Drapeau C.M., et. al.: The novel influenza A (H1N1) virus pandemic: an update. Ann Thorac Med 2009; 4: pp. 163-172.
5. Sullivan S.J., Jacobson R.M., Dowdle W.R., et. al.: 2009 H1N1 Influenza. Mayo Clin Proc 2010; 85: pp. 64-76.
6. Reittner P., Ward S., Heyneman L., et. al.: Pneumonia: high-resolution CT findings in 114 patients. Eur Radiol 2003; 13: pp. 515-521.
7. Agarwal P.P., Cinti S., Kazerooni E.A.: Chest radiographic and CT findings in novel swine-origin influenza A (H1N1) virus (S-OIV) infection. AJR Am J Roentgenol 2009; 193: pp. 1488-1493.
8. Garcia-Garcia J., Ramos C.: Influenza, an existing public health problem [article in Spanish]. Salud Publica Mex 2006; 48: pp. 244-267.
9. Bay A., Etlik O., Oner A.F., et. al.: Radiological and clinical course of pneumonia in patients with avian influenza H5N1. Eur J Radiol 2007; 61: pp. 245-250.
10. Dawood F.S., Jain S., Finelli L., et. al.: Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med 2009; 360: pp. 2605-2615.
11. Chowell G., Bertozzi S.M., Colchero M.A., et. al.: Severe respiratory disease concurrent with the circulation of H1N1 influenza. N Engl J Med 2009; 361: pp. 674-679.
12. Ajlan A.M., Quiney B., Nicolaou S., et. al.: Swine-origin influenza A (H1N1) viral infection: radiographic and CT findings. AJR Am J Roentgenol 2009; 193: pp. 1494-1499.
13. Lee C.W., Seo J.B., Song J.W., et. al.: Pulmonary complication of novel influenza A (H1N1) infection: imaging features in two patients. Kor J Radiol 2009; 10: pp. 531-534.
14. Marchiori E, Zanetti G, Hochhegger B, et al. High-resolution computed tomography findings from adult patients with influenza A (H1N1) virus-associated pneumonia. Eur J Radiol. In press.
15. Rossi S.E., Erasmus J.J., Volpacchio M., et. al.: “Crazy-paving” pattern at thin-section CT of the lungs: radiologic-pathologic overview. Radiographics 2003; 23: pp. 1509-1519.
16. Fisman D.N., Savage R., Gubbay J., et. al.: Older age and a reduced likelihood of 2009 H1N1 virus infection. N Engl J Med 2009; 361: pp. 2000-2001.