
Rationale and Objectives
The aim of this study was to describe the mammographic, sonographic, and magnetic resonance imaging (MRI) findings of micropapillary ductal carcinoma in situ.
Materials and Methods
Between May 2004 and April 2008, the pathology database of a single institution was reviewed for patients diagnosed with histologically proven DCIS with a predominant micropapillary component. Clinical data and preoperative imaging studies, including mammography, sonography, and/or MRI, were reviewed.
Results
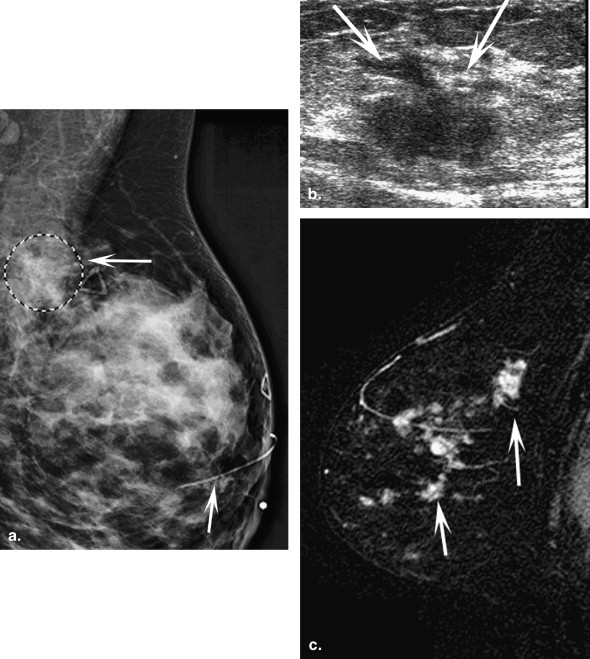
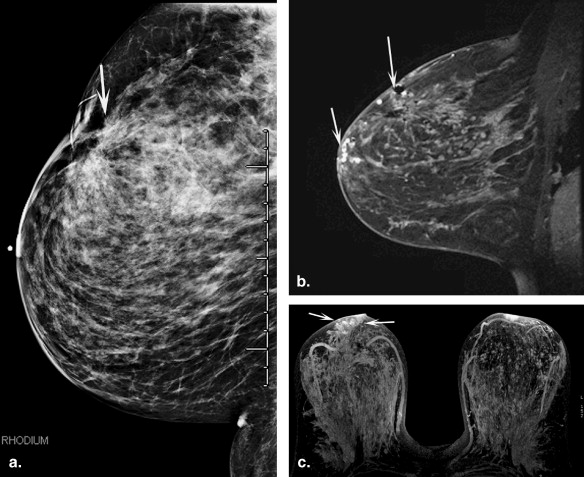
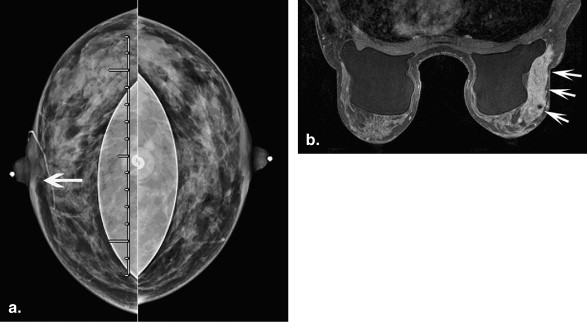
Forty-one patients (mean age, 55 years; range, 33–82 years) with 42 tumors were included in this study. Most tumors ( n = 32 [76%]) were detected on screening mammography, with a mean tumor size of 4.7 cm (range, 0.5–13 cm). Of 42 tumors, seven (16%) were multicentric, and 23 (54%) were high nuclear grade. Calcifications were identified in 36 tumors (86%) on mammography, most frequently with pleomorphic morphology (15 tumors [42%]). Sonography was frequently normal (17 of 36 [47%]). When abnormal, irregular mass and angular margins were the most common sonographic features. All four tumors with MRI showed non-mass-like enhancement and showed the best correlation with pathologic size.
Conclusions
Micropapillary ductal carcinoma in situ is a unique subset of in situ cancer that is frequently clinically occult but has a large mean size at diagnosis and demonstrates highly suspicious features at imaging including pleomorphic calcifications on mammography and an irregular mass at sonography. MRI may be the imaging modality of choice for delineation of disease extent and warrants further validation.
Ductal carcinoma in situ (DCIS) is heterogeneous in histopathologic characteristics and biologic behavior . With the increased use of screening mammography, DCIS now accounts for 22% to 45% of breast cancers detected in patients undergoing biopsy for clinically occult lesions seen on mammography . Micropapillary DCIS is a subtype of DCIS characterized by the presence of papillary fronds that protrude into the ductal lumen in a regular distribution . This subtype of DCIS is frequently multifocal and multicentric, which may lead to underestimation of size by imaging modalities. Therefore, Scott et al proposed to separate pure cases of micropapillary DCIS to accrue prognostic information.
It is well documented that breast-conserving surgery followed by external-beam radiation is associated with a low rate of local recurrence, and survival is equivalent to treatment by mastectomy . Preoperative estimation of tumor size by mammography, sonography, and in some instances magnetic resonance imaging (MRI) is important in surgical planning to achieve histologic negative margins . Mammography has been shown to underestimate the histologic size of DCIS . The extent of size discrepancy was related to the histologic type of DCIS, the size of the micropapillary (cribriform) subtype of DCIS was more commonly underestimated on mammography compared to the comedo subtype, and frequently required one or more additional surgical procedures . To date, there are scant data in the literature describing the imaging characteristics of micropapillary DCIS. With this retrospective study, we aimed to describe the imaging features of micropapillary DCIS.
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Mammography
Get Radiology Tree app to read full this article<
Sonography
Get Radiology Tree app to read full this article<
MRI
Get Radiology Tree app to read full this article<
Image Evaluation
Get Radiology Tree app to read full this article<
Histopathologic Evaluation
Get Radiology Tree app to read full this article<
Results
Clinical Findings and Presentation
Get Radiology Tree app to read full this article<
Table 1
Clinical and Pathological Features in 41 Patients with 42 Micropapillary Ductal Carcinoma in Situ Tumors
Feature_n_ (%) Clinical presentation ( n = 41) Palpable mass 8 (20) Palpable mass with nipple discharge 1 (2) Nipple discharge 1 (2) Asymptomatic 31 (76) Tumor size (cm) ( n = 42) <2 7 (17) 2–5 17 (40) >5–10 13 (31) >10 5 (12) Nuclear grade ( n = 42) 1 and 2 19 (45) 3 23 (55) Estrogen receptor status (n = 42) Positive 35 (83) Negative 5 (12) Not available 2 (5) Progesterone receptor status (n = 42) Positive 28 (67) Negative 12 (29) Not available 2 (5) Human epidermal growth factor receptor 2 status ( n = 42) Positive 3 (7) Negative 5 (12) Not available 34 (81)
Percentages do not add up to 100%, because of rounding.
Get Radiology Tree app to read full this article<
Imaging Findings
Mammography
Get Radiology Tree app to read full this article<
Table 2
Mammographic, Sonographic, and MRI Findings in 42 Patients with Micropapillary Ductal Carcinoma in Situ
Imaging Finding_n_ (%) Mammography ( n = 42) Total calcifications 35 (83) Calcifications only 32 (76) Mass with calcifications 1 (2) Focal asymmetry with calcifications 1 (2) Architectural distortion with calcifications 1 (2) Mass only 3 (7) Focal asymmetry only 2 (5) Ductal dilatation 1 (2) Nipple skin thickening 1 (2) Sonography ( n = 36) Negative 17 (47) Architectural distortion 7 (19) Ductal dilatation 5 (14) Mass 7 (19) Mass characteristics (n = 7) Shape Irregular 5 (71) Oval 2 (19) Margins Indistinct 1 (14) Angular 4 (57) Microlobulated 2 (29) Echogenecity Hypoechoic 7 (100) MRI ( n = 4) Non-mass-like enhancement 4 (100) Distribution Segmental 2 (50) Regional 2 (50) Internal pattern Clumped 3 (75) Heterogeneous 1 (25) Type 1 kinetic curve 2 (50) Type 2 kinetic curve 1 (25) Type 3 kinetic curve 1 (25)
Percentages do not add up to 100%, because of rounding.
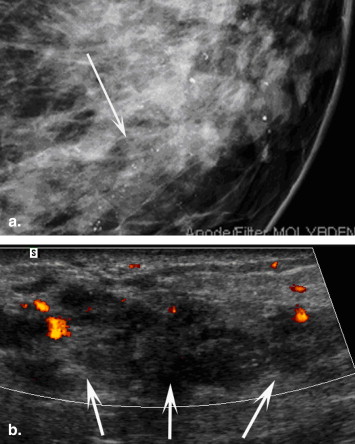
Table 3
Morphology and Distribution of Calcifications in 35 Patients with Micropapillary Ductal Carcinoma in Situ
Distribution Morphology Linear Heterogeneous Pleomorphic Amorphous Punctate Total Segmental 3 1 11 2 17 Grouped 3 4 1 8 Regional 1 4 3 8 Scattered 1 1 2 Total 3 5 15 10 2 35
Get Radiology Tree app to read full this article<
Sonography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Treatment and Histopathologic Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Rosen P.P.: Intraductal carcinoma.Rosen P.P.Rosen’s Breast Pathology.2001.Lippincott Williams &WilkinsPhiladelphia, PA:pp. 257-324.
2. Stomper P.C., Connolly J.L.: Ductal carcinoma in situ of the breast: correlation between mammographic calcification and tumor subtype. AJR Am J Roentgenol 1992; 159: pp. 483-485.
3. Jaffer S., Bleiweiss I.: Histologic classification of ductal carcinoma in situ. Microsc Res Tech 2002; 59: pp. 92-101.
4. Scott M.A., Lagios M.D., Axelsson K., et. al.: Ductal carcinoma in situ of the breast: reproducibility of histological subtype analysis. Hum Pathol 1997; 28: pp. 967-973.
5. Miller A.R., Brandao G., Prihoda T.J., et. al.: Positive margins following surgical resection of breast carcinoma: analysis of pathologic correlates. J Surg Oncol 2004; 86: pp. 134-140.
6. Mirza N.Q., Vlastos G., Meric F., et. al.: Predictors of locoregional recurrence among patients with early-stage breast cancer treated with breast conserving therapy. Ann Surg Oncol 2002; 9: pp. 256-265.
7. Park C.C., Mitsumori M., Nixon A., et. al.: Outcome at 8 years after breast conserving surgery and radiation therapy for invasive breast cancer: influence of margin status and systemic therapy on local recurrence. J Clin Oncol 2000; 18: pp. 1668-1675.
8. Mann R.M., Veltman J., Barentsz J.O., et. al.: The value of MRI compared to mammography in the assessment of tumour extent in invasive lobular carcinoma of the breast. Eur J Surg Oncol 2008; 34: pp. 135-142.
9. Mann R.M., Loo C.E., Wobbes T., et. al.: The impact of preoperative breast MRI on the re-excision rate in invasive lobular carcinoma of the breast. Breast Cancer Res Treat 2010; 119: pp. 415-422.
10. Wasif N., Garreau J., Terando A., et. al.: MRI versus ultrasonography and mammography for preoperative assessment of breast cancer. Am Surg 2009; 75: pp. 970-975.
11. Marcotte-Bloch C, Balu-Maestro C, Chamorey E, et al. MRI for the size assessment of pure ductal carcinoma in situ (DCIS): a prospective study of 33 patients. Eur Radiol. In press.
12. Holland R., Hendriks J.H.: Extent, distribution and mammographic/histological correlations of breast ductal carcinoma in situ. Lancet 1990; 335: pp. 519-522.
13. American College of Radiology: Mammography.Breast Imaging Reporting and Data System (BI-RADS).2003.American College of RadiologyReston, VA:
14. American College of Radiology: Ultrasound.Breast Imaging Reporting and Data System (BI-RADS).2003.American College of RadiologyReston, VA:
15. American College of Radiology: MRI.Breast Imaging Reporting and Data System (BI-RADS).2003.American College of RadiologyReston, VA:
16. Ikeda D.M., Andersson I.: Ductal carcinoma in situ: atypical mammographic appearances. Radiology 1989; 172: pp. 661-666.
17. Dershaw D., Abramson A., Kinne D.W.: Ductal carcinoma in situ: mammographic findings and clinical implications. Radiology 1989; 170: pp. 411-415.
18. Stomper P.C., Connolly J.L., Meyer J.E., et. al.: Clinically occult ductal carcinoma in situ detected with mammography: analysis of 100 cases with radiologic-pathologic correlation. Radiology 1989; 172: pp. 235-241.
19. Schnitt S.J., Silen W., Sadowsky N.L., et. al.: Ductal carcinoma in situ (intraductal carcinoma) of the breast. N Engl J Med 1988; 318: pp. 898-903.
20. Evans A.J., Pinder S., Ellis I.O., et. al.: Screening-detected and symptomatic ductal carcinoma in situ: mammographic features with pathologic correlation. Radiology 1994; 191: pp. 237-240.
21. Shin H.J., Kim H.H., Kim S.M., et. al.: Screening-detected and symptomatic ductal carcinoma in situ: Differences in the sonographic and pathologic features. AJR Am J Roentgenol 2008; 190: pp. 516-525.
22. Moon W.K., Myung J.S., Lee Y.J., et. al.: US of ductal carcinoma in situ. Radiographics 2002; 22: pp. 269-281.
23. Yang W.T., Tse M.K.: Sonographic, mammographic, and histopathologic correlation of symptomatic ductal carcinoma in situ. AJR Am J Roentgenol 2004; 182: pp. 101-110.
24. Tohno E.Cosgrove D.O.Sloane D.P.Ultrasound Diagnosis of Breast Diseases.1994.Churchill LivingstoneLondon, UK:pp. 178-179.
25. Stavros A.T.: Ultrasound of ductal carcinoma in situ.Silverstein M.J.Ductal Carcinoma in Situ of the Breast.1997.Williams & WilkinsBaltimore, MD:pp. 135-158.
26. Rosen E.L., Smith-Foley S.A., DeMartini W.B., et. al.: BI-RADS MRI enhancement characteristics of ductal carcinoma in situ. Breast J 2007; 13: pp. 545-550.
27. Jansen S.A., Newstead G.M., Abe H., et. al.: Pure ductal carcinoma in situ: kinetic and morphologic MR characteristics compared with mammographic appearance and nuclear grade. Radiology 2007; 245: pp. 684-691.
28. Kuhl C.K., Schrading S., Bieling H.B., et. al.: MRI for diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet 2007; 11: pp. 485-492.
29. Kim D.Y., Moon W.K., Cho N., et. al.: MRI of the breast for the detection and assessment of the size of ductal carcinoma in situ. Korean J Radiol 2007; 8: pp. 32-39.
30. Hung W.K., Ying M., Chan M., et. al.: The impact of sentinel lymph node biopsy in patients with a core biopsy diagnosis of ductal carcinoma in situ. Breast Cancer 2010; 17: pp. 276-280.