
Rationale and Objectives
The aim of this study was to describe the imaging appearance of patients undergoing active surveillance for ductal carcinoma in situ (DCIS).
Materials and Methods
We retrospectively identified 29 patients undergoing active surveillance for DCIS from 2009 to 2014. Twenty-two patients (group 1) refused surgery or were not surgical candidates. Seven patients (group 2) enrolled in a trial of letrozole and deferred surgical excision for 6–12 months. Pathology and imaging results at the initial biopsy and follow-up were recorded.
Results
In group 1, the median follow-up was 2.7 years (range: 0.6–13.9 years). Fifteen patients (68%) remained stable. Seven patients (32%) underwent additional biopsies with invasive ductal carcinoma diagnosed in two patients after 3.9 and 3.6 years who developed increasing calcifications and new masses. In group 2, one patient (14%) was upstaged to microinvasive ductal carcinoma at surgery. Among the patients in both groups with calcifications ( n = 26), there was no progression to invasive disease among those with stable (50%, 13/26) or decreased (19%, 5/26) calcifications.
Conclusions
Among a DCIS active surveillance cohort, invasive disease progression presented as increasing calcifications and a new mass following more than 3.5 years of stable imaging. In contrast, there was no progression to invasive disease among cases of DCIS with stable or decreasing calcifications. Close imaging is a key follow-up component in active surveillance.
Introduction
Since the widespread adoption of screening mammography, the detection of ductal carcinoma in situ (DCIS) has steadily increased, now representing 20%–30% of all new breast cancer diagnoses . Although DCIS is very common, the natural history of the disease is not well known because complete surgical excision is currently the standard of care . However, there is strong circumstantial evidence that 50%–85% of DCIS cases will never progress to invasive disease , and if DCIS does progress, it is unlikely to shift to a higher nuclear grade . This finding has prompted growing concerns regarding DCIS overdiagnosis and overtreatment with a desire for alternative management strategies .
Active surveillance is a management strategy for low-risk DCIS, which avoids surgical excision, may utilize hormonal therapy to suppress growth, and emphasizes imaging follow-up to detect whether progression to invasive disease occurs . Active surveillance is based on the premise that not all DCIS cases are life threatening and that many patients may die with the disease than from the disease, especially those with competing mortality risks . The safety and effectiveness of active surveillance have been identified as a key research need by the Patient-Centered Outcomes Research Institute and the National Institutes of Health Panel on the Diagnosis and Management of Ductal Carcinoma In Situ . There is only one published manuscript of active surveillance outcomes, which demonstrated feasibility among a well-informed patient population but an increased risk of invasive cancer at surgical excision . There are three active surveillance trials in progress. The LOw Risk DCIS (LORD) trial in Europe compares annual mammography to usual care among women with low-grade DCIS with the primary outcome of ipsilateral invasive cancer . In England, the LOw RISk DCIS (LORIS) trial is comparing annual mammography to usual care among non–high grade DCIS with the primary outcome of ipsilateral invasive cancer-free survival . In the United States, the Comparison of Operative to Monitoring and Endocrine Therapy (COMET) trial is comparing endocrine therapy with biannual mammography vs usual care with ipsilateral invasive cancer diagnosis as the primary outcome .
Get Radiology Tree app to read full this article<
Materials and Methods
Case Selection
Get Radiology Tree app to read full this article<
Medical Record Review
Get Radiology Tree app to read full this article<
Imaging Review
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Demographics and DCIS Characteristics Among Patients Undergoing Active Surveillance Because of Medical Comorbidities or Personal Preference (Group 1) and as Part of a Single-arm Trial of Letrozole for 6–12 Months Followed by Surgical Excision (Group 2)
Group 1
n (%) Group 2
Mean (Range)/ n (%) Total 22 7 Age at diagnosis (y, mean [range]) 61.1 (40.8–88.8) 62.5 (50.8–70.6) Race White or Caucasian 13 (59) 5 (71) Black or African American 3 (14) 2 (29) Unavailable or other 6 (28) 0 (0) Follow-up duration (y, median [range]) 2.7 (0.6–13.9) 0.8 (0.6–0.9) Imaging presentation Calcifications on MG 19 (86) 7 (100) Nonmass enhancement on MRI 2 (9) 0 (0) Focal asymmetry on MG 1 (5) 0 (0) Tumor grade Low 1 (5) 0 (0) Intermediate 11 (50) 3 (43) High 9 (41) 4 (57) Missing 1 (5) 0 (0) ER status Positive 20 (91) 7 (100) Negative 0 (0) 0 (0) Missing 2 (9) 0 (0) PR status Positive 15 (68) 5 (71) Negative 5 (23) 2 (29) Missing 2 (9) 0 (0) Hormonal therapy Letrozole 9 (41) 7 (100) Tamoxifen 7 (32) 0 (0) None 6 (27) 0 (0)
ER, estrogen receptor; MG, mammography; MRI, magnetic resonance imaging; PR, progesterone receptor.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Imaging Features and Outcomes of Patients Who Underwent Additional Biopsies During Active Surveillance
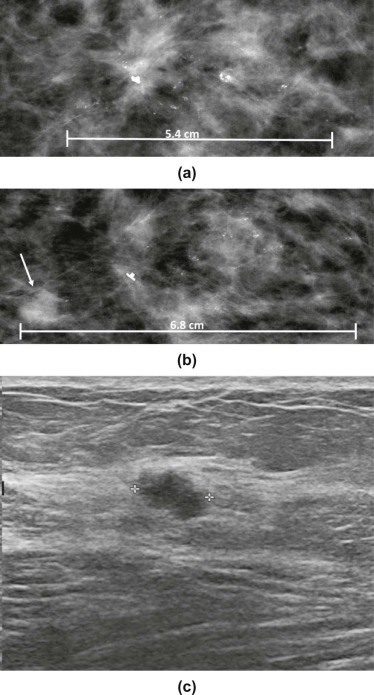
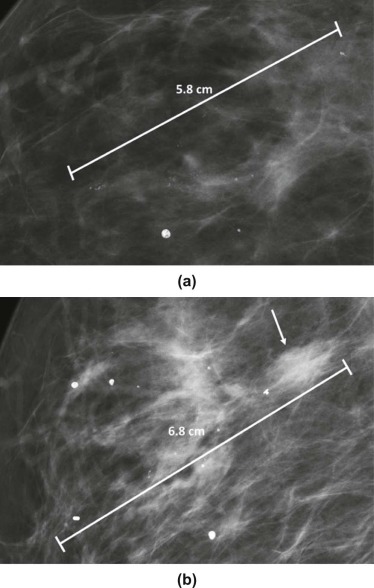
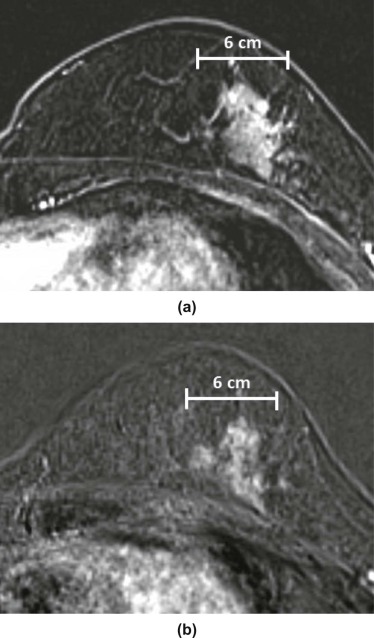
Patient Initial DCIS Pathology Initial Imaging Appearance Therapy Change Prompting Biopsy Follow-up Time (y) Biopsy Results Subsequent Plan 1 ER+, PR+, high grade MG: 5.4 cm of pleomorphic, segmental calcifications Letrozole MG: increased calcifications (6.8 cm) and new mass (0.8 cm) 3.9 IDC: ER+, PR+, HER2+, high grade Lumpectomy: 3.0 cm of IDC 2 ER+, PR+, high grade MG: 6.5 cm of pleomorphic, segmental calcifications Letrozole MG: increased calcifications (8.5 cm) and new mass (1.8 cm) 3.6 IDC: ER+, PR+, HER2−, high grade Mastectomy: 3.0 cm of IDC 3.1 † ER+, PR−, intermediate grade MRI: 1.5 cm (largest site) of clumped, multiple regions of NME Tamoxifen MRI: increased size of one site of NME (1.4 cm, previously 0.7 cm) 4.3 “Benign” \* Return to active surveillance 3.2 † MG: increased number of calcifications 5.2 DCIS: ER+, PR+ Return to active surveillance 3.3 † MRI: new site (0.8 cm) of NME 6.8 Flat epithelial atypia Return to active surveillance—12.9 years of follow-up 4.1 † ER+, PR+, intermediate grade MG: 5.6 cm of pleomorphic, linear calcifications Tamoxifen MRI: new mass (0.9 cm) 0.7 Atypical ductal hyperplasia Return to active surveillance 4.2 † MRI: increased size of mass (1.0 cm) in 4.1 2.5 DCIS: ER+, PR+, high grade Return to active surveillance 4.3 † US: new mass (0.7 cm) 3.3 Stromal fibrosis Return to active surveillance—8.5 years of follow-up 5 ER+, PR−, high grade MG: 3.2 cm of linear, segmental calcifications Letrozole US: new mass (1.0 cm) 1.5 Atypical papilloma Return to active surveillance—3.0 years of follow-up 6 ER+, PR−, high grade MRI: 3.7 cm of clumped, regional NME Letrozole MRI: increased NME (4.7 cm)
US: mass (0.9 cm) 0.5 Atypia suspicious for DCIS Return to active surveillance—1.5 years of follow-up 7 ER and PR missing, intermediate grade MG: 8.0 cm of amorphous, regional calcifications None MG: stable calcifications, questionable asymmetry per the referring surgeon 0.3 Atypical ductal and lobular hyperplasia Return to active surveillance—0.4 years of follow-up
DCIS, ductal carcinoma in situ; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; IDC, invasive ductal carcinoma; MG, mammogram; MRI, magnetic resonance imaging; NME, nonmass enhancement; PR, progesterone receptor; US, ultrasound.
Note: Measurements refer to the long axis.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Progression to Invasive Disease
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Underestimation of the Disease
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Changes to Calcifications Over Time
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Virnig B.A., Tuttle T.M., Shamliyan T., et. al.: Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes. J Natl Cancer Inst 2010; 102: pp. 170-178.
2. Kopans D.B., Smith R.A., Duffy S.W.: Mammographic screening and “overdiagnosis.”. Radiology 2011; 260: pp. 616-620.
3. Sorum R., Hofvind S., Skaane P., et. al.: Trends in incidence of ductal carcinoma in situ: the effect of a population-based screening programme. Breast 2010; 19: pp. 499-505.
4. van Luijt P.A., Fracheboud J., Heijnsdijk E.A., et. al.: Nation-wide data on screening performance during the transition to digital mammography: observations in 6 million screens. Eur J Cancer 2013; 49: pp. 3517-3525.
5. Ernster V.L., Barclay J., Kerlikowske K., et. al.: Incidence of and treatment for ductal carcinoma in situ of the breast. JAMA 1996; 275: pp. 913-918.
6. Mitchell K.B., Kuerer H.: Ductal carcinoma in situ: treatment update and current trends. Curr Oncol Rep 2015; 17: pp. 48.
7. Lopez-Garcia M.A., Geyer F.C., Lacroix-Triki M., et. al.: Breast cancer precursors revisited: molecular features and progression pathways. Histopathology 2010; 57: pp. 171-192.
8. Erbas B., Provenzano E., Armes J., et. al.: The natural history of ductal carcinoma in situ of the breast: a review. Breast Cancer Res Treat 2006; 97: pp. 135-144.
9. Page D.L., Dupont W.D., Rogers L.W., et. al.: Intraductal carcinoma of the breast: follow-up after biopsy only. Cancer 1982; 49: pp. 751-758.
10. Eusebi V., Feudale E., Foschini M.P., et. al.: Long-term follow-up of in situ carcinoma of the breast. Semin Diagn Pathol 1994; 11: pp. 223-235.
11. Rosen P., Snyder R.E., Foote F.W., et. al.: Detection of occult carcinoma in the apparently benign breast biopsy through specimen radiography. Cancer 1970; 26: pp. 944-952.
12. Millis R.R., Barnes D.M., Lampejo O.T., et. al.: Tumour grade does not change between primary and recurrent mammary carcinoma. Eur J Cancer 1998; 34: pp. 548-553.
13. Bijker N., Peterse J.L., Duchateau L., et. al.: Histological type and marker expression of the primary tumour compared with its local recurrence after breast-conserving therapy for ductal carcinoma in situ. Br J Cancer 2001; 84: pp. 539-544.
14. Bleyer A., Welch H.G.: Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med 2012; 367: pp. 1998-2005.
15. Meyerson A.F., Lessing J.N., Itakura K., et. al.: Outcome of long term active surveillance for estrogen receptor-positive ductal carcinoma in situ. Breast 2011; 20: pp. 529-533.
16. Francis A., Fallowfield L., Rea D.: The LORIS Trial: addressing overtreatment of ductal carcinoma in situ. Clin Oncol (R Coll Radiol) 2015; 27: pp. 6-8.
17. Elshof L.E., Tryfonidis K., Slaets L., et. al.: Feasibility of a prospective, randomised, open-label, international multicentre, phase III, non-inferiority trial to assess the safety of active surveillance for low risk ductal carcinoma in situ—The LORD study. Eur J Cancer 2015; 51: pp. 1497-1510.
18. Welch H.G., Black W.C.: Using autopsy series to estimate the disease “reservoir” for ductal carcinoma in situ of the breast: how much more breast cancer can we find?. Ann Intern Med 1997; 127: pp. 1023-1028.
19. Ryser M.D., Worni M., Turner E.L., et. al.: Outcomes of active surveillance for ductal carcinoma in situ: a computational risk analysis. J Natl Cancer Inst 2016; 108:
20. Kuerer H.M.: Ductal carcinoma in situ: treatment or active surveillance?. Expert Rev Anticancer Ther 2015; 15: pp. 777-785.
21. Gierisch J.M., Myers E.R., Schmit K.M., et. al.: Prioritization of research addressing management strategies for ductal carcinoma in situ. Ann Intern Med 2014; 160: pp. 484-491.
22. Allegra C.J., Aberle D.R., Ganschow P., et. al.: National Institutes of Health State-of-the-Science Conference statement: diagnosis and management of ductal carcinoma in situ September 22–24, 2009. J Natl Cancer Inst 2010; 102: pp. 161-169.
23. Francis A., Thomas J., Fallowfield L., et. al.: Addressing overtreatment of screen detected DCIS; the LORIS trial. Eur J Cancer 2015; 51: pp. 2296-2303.
24. Patient-Centered Outcomes Research Institute : Comparison of Operative versus Medical Endocrine Therapy for Low Risk DCIS: The COMET Trial. Available at http://www.pcori.org/research-results/2016/comparison-operative-versus-medical-endocrine-therapy-low-risk-dcis-comet Accessed August 8, 2016
25. Letrozole in Treating Postmenopausal Women With Ductal Carcinoma in Situ. Available at https://ClinicalTrials.gov/ct2/show/NCT01439711 Accessed May 13, 2016
26. Ikeda D.M., Hylton N.M., Kuhl C.K., et. al.: BI-RADS: mammography.D’Orsi C.J.Mendelson E.B.Ikeda D.M. et. al.Breast Imaging Reporting and Data System: ACR BI-RADS—Breast Imaging Atlas.2013.American College of RadiologyReston, VA:
27. Brennan M.E., Turner R.M., Ciatto S., et. al.: Ductal carcinoma in situ at core-needle biopsy: meta-analysis of underestimation and predictors of invasive breast cancer. Radiology 2011; 260: pp. 119-128.
28. Liberman L., Hann L.E., Dershaw D.D., et. al.: Mammographic findings after stereotactic 14-gauge vacuum biopsy. Radiology 1997; 203: pp. 343-347.
29. Barreau B., de Mascarel I., Feuga C., et. al.: Mammography of ductal carcinoma in situ of the breast: review of 909 cases with radiographic-pathologic correlations. Eur J Radiol 2005; 54: pp. 55-61.
30. Yamada T., Mori N., Watanabe M., et. al.: Radiologic-pathologic correlation of ductal carcinoma in situ. Radiographics 2010; 30: pp. 1183-1198.
31. Chen Y.Y., DeVries S., Anderson J., et. al.: Pathologic and biologic response to preoperative endocrine therapy in patients with ER-positive ductal carcinoma in situ. BMC Cancer 2009; 9: pp. 285.
32. Soumian S., Verghese E.T., Booth M., et. al.: Concordance between vacuum assisted biopsy and postoperative histology: implications for the proposed Low Risk DCIS Trial (LORIS). Eur J Surg Oncol 2013; 39: pp. 1337-1340.
33. Li J.J., Chen C., Gu Y., et. al.: The role of mammographic calcification in the neoadjuvant therapy of breast cancer imaging evaluation. PLoS ONE 2014; 9: e88853
34. Adwani A., Lowe S., Ebbs S.R.: Disappearing microcalcification after neoadjuvant chemotherapy—a case report. Eur J Surg Oncol 2000; 26: pp. 98-100.
35. Weiss A., Lee K.C., Romero Y., et. al.: Calcifications on mammogram do not correlate with tumor size after neoadjuvant chemotherapy. Ann Surg Oncol 2014; 21: pp. 3310-3316.
36. Adrada B.E., Huo L., Lane D.L., et. al.: Histopathologic correlation of residual mammographic microcalcifications after neoadjuvant chemotherapy for locally advanced breast cancer. Ann Surg Oncol 2015; 22: pp. 1111-1117.
37. Taylor C., Georgian-Smith D.: Regression of breast cancer in four patients treated with tamoxifen: mammographic features. AJR Am J Roentgenol 1994; 162: pp. 613-616.
38. Seymour H.R., Cooke J., Given-Wilson R.M.: The significance of spontaneous resolution of breast calcification. Br J Radiol 1999; 72: pp. 3-8.